Overall, medical school is pretty great. At least that's what I keep telling myself. The workload is insane, your world gets reduced to things in and around med school, the debt is.. well we just won't even go there. But it's a worthwhile endeavor, and you tend to feel accomplished when you pass your exams or impress your clinical leaders. And you're surrounded by 100+ people all doing the same thing, so there's a sense of camaraderie (the people in our class are pretty awesome).
However, I do have one criticism, one qualm if you will, about medical school, and it is this: you constantly feel like you're being thrown from one thing to the next. Unfortunately, I don't really see any alternative. Originally I planned on writing about how the layout and culture of medical education promote this shuttling behavior, and how it hurts students in both the short term and long term. After thinking about it though, I don't really see what could be different. Medical school year one is a strange place. The first semester, you barrel through biochem and anatomy while starting your intro to medicine and problem based learning classes. The sciences are particularly guilty of moving from topic to topic. Granted, they have a lot of material to cover. Unfortunately, you almost constantly feel that by the time you master something, you have two or three new things to do (if you're lucky, only two or three things).
Additionally, you're often shuttled from one topic you've never encountered before to another topic you've never encountered before. The intro medicine class is very guilty of this. For example, we interviewed our first real patients as part of the class. We did this without really knowing what we were supposed to accomplish or even how to do it. And this really gets to the root of my criticism. I think the reason we (fine, I) feel like we're bouncing along from one thing to the other is simply because there's an abundance of information, and we haven't yet developed the filters to manage it yet. It's difficult to know what the important parts of biochem and anatomy are because we haven't had an exam to spotlight where the important details are coming from. Intro to medicine is even worse because we have almost zero knowledge about which questions are important and relevant. So, even when we know what to ask, we have no idea why we're doing it. And strangely enough, we won't even get that knowledge until second year, when pathophysiology is discussed.
But, I can see why we do it this way. First, curricula are hard to completely reinvent so we can only reform parts at a time. Plus people dislike change; blame it on the humans. Second, you can't filter information if you don't have any to start with. If I don't learn how to take a detailed history, I won't know which parts I can skip over or include. If I don't memorize the muscles and there innervations, I won't have the information to make a diagnosis. If I don't know how the cell membrane is affected by deviations in extracellular potassium... well, that one is stretching it. Ultimately, we just have to run the gauntlet and assume/tell ourselves it will work out in the end.
Thursday, September 6, 2012
Monday, August 27, 2012
What Beautiful Anatomy You Have
Med school marches onward, seemingly oblivious to the poor souls it's dragging with it. Realistically, we are a boiler, gradually building up pressure until that first exam hits and we burst out the safety release valve. That will be an interesting day for sure.
This week was notable for our first anatomy dissection. Every med school I know of has a cadaver dissection as part of the course, the point being to help us learn anatomy. To say it is an odd experience is downplaying it rather substantially. For one, death is not a topic that is addressed in casual conversation, thus evoking some anxious feelings when it is presented in such an explicit form. Additionally, cutting apart the flesh of the deceased is surreal. Generally, we tend to discourage stabbing other humans with scalpels and scissors and other pointy objects. Making cuts into the body requires you to fight back against decades of rule governed behavior, and even when you do, you still get the feeling that something is amiss. Yet, I certainly wouldn't pass up the opportunity to do dissections, and I know my classmates feel the same way.
Even though we've only had one dissection (two more this week; not sure what we did to earn this punishment), I've already learned a great deal. We started with the back because the muscles are large and it's relatively difficult to screw it up. To get to the good stuff however, required several hours of removing fat from the body spaces. Our body, unfortunately, is quite obese, which essentially acts to increase the amount of time it takes us to remove unimportant parts and ramps up the difficulty in defining the stuff we do want to keep. The other problem with dissection is that most anatomy atlases are color coded. This is great for learning initially, but completely useless for the cadaver. Normal living tissue retains some of its color, but the cadavers are mostly shades of gray. And since part of our grade comes from identifying structures on cadavers, it's kind of a big deal to know what areas you are dealing with.
I'm going to try to touch on some non-med school related topics this week, but we'll see how that actually goes. Now that we're done with orientation, our schedule is a little more regular. Apparently things don't really die down until the spring semester though, so I'm SOL at the moment. Is it too late to change to business school?
I'm going to try to touch on some non-med school related topics this week, but we'll see how that actually goes. Now that we're done with orientation, our schedule is a little more regular. Apparently things don't really die down until the spring semester though, so I'm SOL at the moment. Is it too late to change to business school?
Saturday, August 18, 2012
Applying to Medical School: Skillful Interviewing
For those of you applying to medical school, we're nearing the point where the first interviews will begin. Typically, the first invites go out in late July/August, and the first interviews are in September. Each school is different, particularly depending on when the secondary application goes out. Anyways, the interview is probably the most important part of the admissions process. Why? If a school gives you an interview, they're already pretty interested in you. Remember, only 10-20% of applicants to a school are interviewed. You already beat out a large portion of people. Now you have to land the deal.
In terms of helping or hurting you, the interview can do both, but to different levels. My opinion is that, a good interview will help you a little, but a bad interview will hurt you a lot. Think of it this way: You are like a cake. When you go to interview, the admissions committee is looking to confirm that you are what they want. They are checking to see if the cake is ready and looks good. Your individual talents/personality is the frosting or sprinkles or design that sets the cake apart from others. However, if they find your cake lacking in substance or taste, no matter how much frosting you put on it, no one will want to eat it.
So, how do you make sure you present your best, most tastiest cake? First and foremost, acknowledge that there is a great degree of luck involved. For example, on one interview, my interviewer and I had a lot in common. As a result, the interview flowed nicely from topic to topic, and we both had fun (at least I did). That was the luck factor; so much is dependent on who your interviewer is and how he/she is feeling that day, among other things. Don't despair though! You can still nail the interview by doing a few simple things.
1. Look nice. Make sure you are dressed nicely (suit is highly recommended) and well groomed. Medicine is fairly conservative (at least the interview part), so don't go overboard on make-up or fashion.
2. Be comfortable and relaxed. Okay, realistically you'll be pretty anxious; I was too. Just try not to let it show too much. Do some deep breathing exercises if you find yourself getting too worked up. And don't be afraid to take a second or two to think about a question before you respond. You want your sentences to be of substance; talking more doesn't necessarily mean better. Also, I recommend you wear your suit a couple times before your interview day. You can tell who is wearing a suit for the first time because they tend to look uncomfortable. So dress up to class or work a couple times to get used to the feel.
3. Be polite and positive. This goes without saying. Be polite to everyone, especially the staff and other interviewees. You never know when you are being observed...
4. Be passionate, be genuine, and know your application material. This is crucial. You will probably be asked about your application (some interviews are different, like the MMI). Make sure you can spend at least a few minutes talking about anything you mentioned. Most importantly, make sure you speak enthusiastically. Now, you don't want to go used-car-salesman on your interviewer, but make sure you convey a degree of excitement about the things you mentioned in your application. Look, everyone knows there is a great deal of scut work you have to do to get into med school. Just don't present that way. If you did research, talk about it. If you had a powerful experience volunteering or on a trip, explain how it impacted you so heavily. It's not the smartest, most accomplished people who get into medical school. It's the ones who show that they want it most, that they're willing to put in the effort to succeed. Make damn sure you get that point across.
5. Send a thank you note. For the love of all things good, write down the name of your interviewer(s) so you can send a thank you note. Often times you'll send it to the admissions office, and they can forward it to the person. Very important you do this. It doesn't have to be long (mine was a couple sentences saying thank you and mentioning a specific thing we talked about to make it seem less generic), but it's important you do this follow up.
You can find interview tips just by doing a simple Google search, so I encourage you to look up those general pointers. Honestly, the medical school interview is a lot of fun. It's the closest you'll be to getting into med school. You'll get to talk to students, find out about the curriculum, maybe even sit in on a lecture (if you get the option to stay with a student host, do it. It's way better than staying in a hotel. Just trust me on this one). The interview is the final hurdle you have to get over. There is essentially nothing left to do afterwards except wait for a decision. You can send update letters or interest letters to the school, but make sure you actually have something substantial to say. Avoid calling the office to see if a decision is made; you'll find out in due time. Most importantly, relax a bit. You got through it all! If all goes well, you'll get that beautiful, wonderful acceptance letter (and often phone call) in no time.
So remember, have fun. It's a long, tedious, stressful process, but if you stay positive and make the most of it, it'll reflect in your application, and good things will happen.
So, how do you make sure you present your best, most tastiest cake? First and foremost, acknowledge that there is a great degree of luck involved. For example, on one interview, my interviewer and I had a lot in common. As a result, the interview flowed nicely from topic to topic, and we both had fun (at least I did). That was the luck factor; so much is dependent on who your interviewer is and how he/she is feeling that day, among other things. Don't despair though! You can still nail the interview by doing a few simple things.
1. Look nice. Make sure you are dressed nicely (suit is highly recommended) and well groomed. Medicine is fairly conservative (at least the interview part), so don't go overboard on make-up or fashion.
2. Be comfortable and relaxed. Okay, realistically you'll be pretty anxious; I was too. Just try not to let it show too much. Do some deep breathing exercises if you find yourself getting too worked up. And don't be afraid to take a second or two to think about a question before you respond. You want your sentences to be of substance; talking more doesn't necessarily mean better. Also, I recommend you wear your suit a couple times before your interview day. You can tell who is wearing a suit for the first time because they tend to look uncomfortable. So dress up to class or work a couple times to get used to the feel.
3. Be polite and positive. This goes without saying. Be polite to everyone, especially the staff and other interviewees. You never know when you are being observed...
4. Be passionate, be genuine, and know your application material. This is crucial. You will probably be asked about your application (some interviews are different, like the MMI). Make sure you can spend at least a few minutes talking about anything you mentioned. Most importantly, make sure you speak enthusiastically. Now, you don't want to go used-car-salesman on your interviewer, but make sure you convey a degree of excitement about the things you mentioned in your application. Look, everyone knows there is a great deal of scut work you have to do to get into med school. Just don't present that way. If you did research, talk about it. If you had a powerful experience volunteering or on a trip, explain how it impacted you so heavily. It's not the smartest, most accomplished people who get into medical school. It's the ones who show that they want it most, that they're willing to put in the effort to succeed. Make damn sure you get that point across.
5. Send a thank you note. For the love of all things good, write down the name of your interviewer(s) so you can send a thank you note. Often times you'll send it to the admissions office, and they can forward it to the person. Very important you do this. It doesn't have to be long (mine was a couple sentences saying thank you and mentioning a specific thing we talked about to make it seem less generic), but it's important you do this follow up.
You can find interview tips just by doing a simple Google search, so I encourage you to look up those general pointers. Honestly, the medical school interview is a lot of fun. It's the closest you'll be to getting into med school. You'll get to talk to students, find out about the curriculum, maybe even sit in on a lecture (if you get the option to stay with a student host, do it. It's way better than staying in a hotel. Just trust me on this one). The interview is the final hurdle you have to get over. There is essentially nothing left to do afterwards except wait for a decision. You can send update letters or interest letters to the school, but make sure you actually have something substantial to say. Avoid calling the office to see if a decision is made; you'll find out in due time. Most importantly, relax a bit. You got through it all! If all goes well, you'll get that beautiful, wonderful acceptance letter (and often phone call) in no time.
So remember, have fun. It's a long, tedious, stressful process, but if you stay positive and make the most of it, it'll reflect in your application, and good things will happen.
Sunday, August 12, 2012
Return From Hiatus, With A Bright White Coat
Despite having nearly nothing to do for the past few weeks, I just could not find time to write a new post. It is truly a tragedy. Anyways, some things have changed since we last spoke. Most notably, I have made the transition from premed student to medical student. This was accomplished through a symbolic and somewhat odd ceremony called the White Coat Ceremony. Like a mini-graduation, several of the deans spoke to us and our family/friends/passing hobos about the significance of the occasion and offered advice about how to proceed forward. Then, four at a time, we are called up to the stage and "coated" by one of the deans. This was followed by a recitation of a modified version of the Hippocratic Oath, which was followed (I think) by drinking.
The odd part of the ceremony was two-fold. First, it was inordinately humid out, so everyone was drenched in sweat by the time we finished. Secondly, it seemed strange to hold such an elaborate celebration before we actually accomplished anything. Don't get me wrong, we all got into med school, which is a feat on its own. But I think the ceremony would make more sense between the 2nd and 3rd year. That's the bigger transition, when you go from student in lecture to student in practice.
Regardless, the start of school is still something to be excited about. Unfortunately, most of the week was spent in orientation type events, so we've yet to dive in deep (that changes starting tomorrow). So, what do I have on my plate for the next few months? Well, I've got your standard biochemistry and anatomy courses. We also have two courses in public health and human behavior, one each. Finally, we have a couple clinical med and problem based learning courses. At first glance, it may seem like your ordinary (difficult) college schedule. The deceptive part is that we have multiple lectures per subject per day. For example, tomorrow I have a three hour anatomy block, followed by two hours of lectures in biochem and another 1.5 hour public health lecture. That's how they get you. I have 6 hours of biochem, 9 hours of anatomy (lab starts next week), 8.5 hours of public health, and 3 hours of behavior. And that's just lecture time; many more hours of study are required for mastery. I'm starting to get that fire hose analogy now.
Anyways, I'll try to do better about posting. Maybe I'll even get on a schedule. Consistency is key! Here's to the start of an exciting four years!
Saturday, July 21, 2012
We All Spend Time As A Shadow
I leave my apartment and hop in the car, already feeling a little drowsy. It's 10:30 pm, and I'm heading to work. In order to satisfy a requirement for an internship, I scheduled two ED shadowing shifts back to back, starting at 11pm and going till 7am. I took two shifts previously from 6pm to 2am, but this was different. Going to work in the middle of the night feels unnatural, though the commute is pretty good. I arrive at the hospital, carrying my coffee-filled thermos (essential), ready for the night shift.
So, you want to be a doctor. Fantastic (although if I had a nickel for every time I heard that, I wouldn't be taking out so many loans for med school). What does a doctor do? If you answered "Helps people" you are probably a freshman with good intentions but much naïveté. If you chose "Paperwork" or "Sitting at a computer" you probably have a little more experience. If you said "Inflict pain and interrupt frequently" you are probably a patient. Most people have a general idea of what physicians do, but they lack the important day-to-day details. Medicine is fairly romanticized thanks in large part to shows like ER, House, or Grey's Anatomy, and the many that came before it. Watching people put in orders, review charts, wait for labs, or conduct rounds does not make for very interesting TV (to the general public at least). Thus we arrive at our stereotypical freshman pre-med, gunning for med school without any conception of what physicians actually do. This is where shadowing comes in.
The ED is arranged like a giant horseshoe, the interior being the nurses' and physician's stations and the exterior being the patient rooms. I set my coffee down and put my snack in the mini-fridge (god help you if you fail to bring snacks). I greet Dr. S. and we begin the night. Dr. S. is very mild mannered and speaks calmly (ER docs tend to come from both ends of the spectrum, calm and manic). It is a typical night at the ER; abdominal pain is coming at us from every direction and shows no sign of letting up. Not too far into the shift, an elderly woman arrives by EMS. She was unconscious and had some dried blood on her head, suspicious for a fall. She was weakly responsive to pain, but no spontaneous movement or sounds. She got the usual 'ER Special' consisting of IVs, blood tests, and cardiac monitoring. She would almost certainly be admitted. Neurology would be consulted as soon as possible. Several hours later, her daughter came running out of the room, shouting for help; the patient was having a seizure. After a tense minute or two of not being able to locate any nurses or Dr. S. (he is the only physician on at this point), we stream into the room to assess the situation. The patient has stopped seizing at the moment, but is now not breathing. Her heart rate plummets. Quickly, a nurse starts to bag her, and Dr. S. makes the decision to intubate. Respiratory is paged, and a nurse prepares anti-convulsants. Finally, she's stabilized, and we all go back to work. No rest for the weary.
Shadowing is exactly as it sounds: the student follows the physician like a shadow, in order to observe. However, unlike a shadow, you will constantly be in the way, and you can/might be allowed to ask questions. Medical students are expected to ask questions, even if they end up being forced to answer their very own questions and ultimately being chastised for not knowing the answer (doesn't seem fair does it). It is extremely useful though, because you gain firsthand knowledge of how a typical day/shift goes. For example, I was shadowing an ER doc, and for the first 2-3 hours, we didn't see one patient. Labs were backed up and beds were full, so we just sat on our asses until it cleared out a bit. You do get to see procedures and patients (especially in surgery), but the little things are actually the most important. Adcoms want to see that you know what you're in for; the fairy-tale can be your motivation, but you better be prepared for the reality.
Around 5am or so, Dr. S. are seeing a patient about back pain when the intercom clicks on. "All help to triage stat!" the nurse shouts (first time I heard stat used in a serious context). Dr. S. is not phased, and continues to interview the patient. Seconds later, "Physician to triage!" Dr. S. sighs, apologizing to the patient, and we head down the hall to the waiting room (slowly I might add). Before we get there, two beds complete with patients come flying around the corner, pushed by a couple personnel. Both patients were stabbed at a party and had just walked in the front door. Minutes later, a third patient comes in and is wheeled back to an empty bed. The ED goes into lock-down, police are called, vitals and IVs are started, and ambulances are called to transfer the patients (the hospital is not a trauma facility). Shortly after our three stab victims arrive, a code blue goes out over the intercom. The physician covering the wards, Dr. P., is currently in the ED, and Dr. S. is not sure if she's even ACLS certified. Dr. S. and his scribe take off after her with the code box, and I am tasked with getting vitals from the patients. They all appear to be in discomfort, but one looks very pale and is shaking (effects of epinephrine). Dr. S. and his now disheveled looking scribe (CPR will do that to you) return, and the patients are transferred.
So, shadowing is important, an unwritten requirement of medical school. But how do you go about it? I was lucky; I got an internship through the university that handled the initial contact. For those less fortunate, I would suggest asking around the hospital if you volunteer at one. Academic medical centers are probably the best choice because they will be used to having medical students around. Ask your friends too. I came from a completely non-medical family, so I was at a bit of a disadvantage. Many of my friends had physician parents or grandparents, so they became a great source of knowledge. There are lots of guides pertaining to shadowing though, so just search SDN or Google for more in depth advice. You don't have to rack up hours and hours of shadowing, but spend one or two full shifts per specialty. It helps to get some variety as well, but even one experience is better than none. Don't forget to have fun, but make sure you reflect on your experiences too. If you really can't see yourself living that life, it might be time to switch paths. That's what shadowing is for. It wipes away some of the glamour, exposing the realism of clinical practice. It disenchants, leaving only the most dedicated behind to finish the journey to medical school.
The ED is arranged like a giant horseshoe, the interior being the nurses' and physician's stations and the exterior being the patient rooms. I set my coffee down and put my snack in the mini-fridge (god help you if you fail to bring snacks). I greet Dr. S. and we begin the night. Dr. S. is very mild mannered and speaks calmly (ER docs tend to come from both ends of the spectrum, calm and manic). It is a typical night at the ER; abdominal pain is coming at us from every direction and shows no sign of letting up. Not too far into the shift, an elderly woman arrives by EMS. She was unconscious and had some dried blood on her head, suspicious for a fall. She was weakly responsive to pain, but no spontaneous movement or sounds. She got the usual 'ER Special' consisting of IVs, blood tests, and cardiac monitoring. She would almost certainly be admitted. Neurology would be consulted as soon as possible. Several hours later, her daughter came running out of the room, shouting for help; the patient was having a seizure. After a tense minute or two of not being able to locate any nurses or Dr. S. (he is the only physician on at this point), we stream into the room to assess the situation. The patient has stopped seizing at the moment, but is now not breathing. Her heart rate plummets. Quickly, a nurse starts to bag her, and Dr. S. makes the decision to intubate. Respiratory is paged, and a nurse prepares anti-convulsants. Finally, she's stabilized, and we all go back to work. No rest for the weary.
Shadowing is exactly as it sounds: the student follows the physician like a shadow, in order to observe. However, unlike a shadow, you will constantly be in the way, and you can/might be allowed to ask questions. Medical students are expected to ask questions, even if they end up being forced to answer their very own questions and ultimately being chastised for not knowing the answer (doesn't seem fair does it). It is extremely useful though, because you gain firsthand knowledge of how a typical day/shift goes. For example, I was shadowing an ER doc, and for the first 2-3 hours, we didn't see one patient. Labs were backed up and beds were full, so we just sat on our asses until it cleared out a bit. You do get to see procedures and patients (especially in surgery), but the little things are actually the most important. Adcoms want to see that you know what you're in for; the fairy-tale can be your motivation, but you better be prepared for the reality.
Around 5am or so, Dr. S. are seeing a patient about back pain when the intercom clicks on. "All help to triage stat!" the nurse shouts (first time I heard stat used in a serious context). Dr. S. is not phased, and continues to interview the patient. Seconds later, "Physician to triage!" Dr. S. sighs, apologizing to the patient, and we head down the hall to the waiting room (slowly I might add). Before we get there, two beds complete with patients come flying around the corner, pushed by a couple personnel. Both patients were stabbed at a party and had just walked in the front door. Minutes later, a third patient comes in and is wheeled back to an empty bed. The ED goes into lock-down, police are called, vitals and IVs are started, and ambulances are called to transfer the patients (the hospital is not a trauma facility). Shortly after our three stab victims arrive, a code blue goes out over the intercom. The physician covering the wards, Dr. P., is currently in the ED, and Dr. S. is not sure if she's even ACLS certified. Dr. S. and his scribe take off after her with the code box, and I am tasked with getting vitals from the patients. They all appear to be in discomfort, but one looks very pale and is shaking (effects of epinephrine). Dr. S. and his now disheveled looking scribe (CPR will do that to you) return, and the patients are transferred.
So, shadowing is important, an unwritten requirement of medical school. But how do you go about it? I was lucky; I got an internship through the university that handled the initial contact. For those less fortunate, I would suggest asking around the hospital if you volunteer at one. Academic medical centers are probably the best choice because they will be used to having medical students around. Ask your friends too. I came from a completely non-medical family, so I was at a bit of a disadvantage. Many of my friends had physician parents or grandparents, so they became a great source of knowledge. There are lots of guides pertaining to shadowing though, so just search SDN or Google for more in depth advice. You don't have to rack up hours and hours of shadowing, but spend one or two full shifts per specialty. It helps to get some variety as well, but even one experience is better than none. Don't forget to have fun, but make sure you reflect on your experiences too. If you really can't see yourself living that life, it might be time to switch paths. That's what shadowing is for. It wipes away some of the glamour, exposing the realism of clinical practice. It disenchants, leaving only the most dedicated behind to finish the journey to medical school.
Sunday, July 15, 2012
Know The Difference: Heart Attack vs Cardiac Arrest
Welcome to the second installment of "Know the Difference," a series which seeks to clear up common medical misnomers. This week, we're tackling a one of the most prominent naming errors on television (and by extension, the public). The scene is a hospital room, with the patient lying in the bed looking quite unhappy and ill. In walk our doctors, who bear an uncanny resemblance to team featured on House. They chat with the patient briefly, exchange some comical banter with each other, and then the patient takes a turn for the worse. The camera pans up to the cardiac monitor, which shows a complete asystole (flat line). Everyone springs dramatically into action, but one of the doctors commits a medical student faux paus. "She's having a heart attack!" he exclaims, sending a brief jolt of pain to the frontal lobes of the clinical staff watching at home.
So what happened? Basically the hotshot doctor was confusing two conditions, heart attack and cardiac arrest. And since they are treated very differently, it is kind of a big deal to get it right. So how do you tell one from the other?
A cardiac arrest (CA) occurs when the heart is no longer pumping blood. This is determined clinically by checking for a pulse. If it is absent, congratulations; you now have a genuine emergency on your hands. When the heart stops pumping blood, oxygen and nutrients cannot circulate through the body, and waste begins to build up. Without intervention, CA is fatal in a matter of minutes (predominantly due to the lack of oxygen)(1). CA is treated differently depending on the cause and EKG interpretation. For instance, the most common one seen on TV is asystole:
So what happened? Basically the hotshot doctor was confusing two conditions, heart attack and cardiac arrest. And since they are treated very differently, it is kind of a big deal to get it right. So how do you tell one from the other?
A cardiac arrest (CA) occurs when the heart is no longer pumping blood. This is determined clinically by checking for a pulse. If it is absent, congratulations; you now have a genuine emergency on your hands. When the heart stops pumping blood, oxygen and nutrients cannot circulate through the body, and waste begins to build up. Without intervention, CA is fatal in a matter of minutes (predominantly due to the lack of oxygen)(1). CA is treated differently depending on the cause and EKG interpretation. For instance, the most common one seen on TV is asystole:
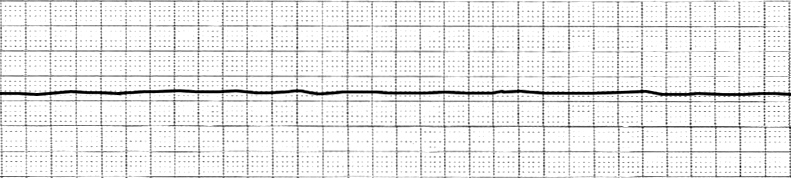 |
| Asystole. Note no discernible waves. Courtesy of wikipedia. |
This is also the most common rhythm seen in Out-of-Hospital arrests(2). Asystole has a number of causes, some reversible some not. Typically, this rhythm is seen after prolonged pulselessness, so the prognosis is grim. The treatment usually involves reversing the underlying condition (toxicity, tamponade, tension pneumo, etc). What it does not involve is electrical shocks. Asystole is not a shockable rhythm. So, while making for very good television, our team of doctors would not be doing any good with the defibrillator in the typical case. Ventricular fibrillation (V-fib or VF) on the other hand, is shockable, even though it may not look like an abnormal rhythm to the untrained eye.
 |
| V-fib. Only random waveforms. Also courtesy of wikipedia. |
VF is a pulseless rhythm where the heart is contracting randomly, out of sync.
A heart attack (MI) is also a serious condition, but does not lead to death per se. An MI occurs when blood flow to the heart is reduced, classically causing chest pain (angina) and dyspnea(2). The reduction of blood flow is usually due to a narrowing in one or more of the coronary arteries. Thus, the primary intervention is to open the arteries back up (PCI) or bypass blocked portions (CABG). The main difference between MI and CA is that cardiac arrest is a complication of an MI. If the blood flow is cut off for too long, heart muscle (myocardium) will die. This can lead to arrhythmias or heart failure, which may lead to death. The EKG of a person having a heart attack can vary substantially, but here are some examples of anterior MIs.
Summary
CA: No pulse, heart is not pumping blood. Rapidly fatal. Treatment (resuscitation) depends on the rhythm appearance.
MI: Reduced blood flow to the heart via the coronary arteries. Muscle death may impair normal function of the heart and lead to death.
So the next time you're watching House or Gray's Anatomy (or ER for the slightly older readers), keep an eye on that monitor and get ready to call those actors out on their mistakes!
Sources
1.CPR - adult. PubMed Health. 2011. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001083/. Accessed July 15, 2012.
2. Mader TJ, et al. Out-of-hospital cardiac arrest outcomes stratified by rhythm analysis. Resuscitation (2012), http://dx.doi.org/10.1016/j.resuscitation.2012.03.033.
3. Heart Attack. PubMed Health. 2011. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001246/. Accessed July 15, 2012.
Monday, July 2, 2012
Behavior's Big Bang Theory
First, I'd like to say my alliteration skills are still spot on. Second, this has nothing to do with the popular TV show, The Big Bang Theory. Sorry to disappoint (secretly I hope I tricked you, and you'll decide to stay anyways).
When I spoke about behavior last time, my discussion was mostly limited to defining what it is and how we look at it. To recap, a behavior is anything you do to solve an adaptive problem, and we categorize it functionally rather than structurally. For example, opening a jar of pickles solves the adaptive problem of getting food, but we don't care exactly how you opened it. You could have twisted the lid off like the majority of individuals (let's be honest, the majority of individuals actually gave it to someone else to open), but you also could have hit the jar with a sledgehammer or treated it to some explosives a la Mythbusters. Each of these techniques would have opened the jar, but some work better than others. The twisting method is quick, easy to do, and requires minimal energy. Blowing up the jar is more pleasing to the senses, but it requires access to explosives and time to set them up, generates new adaptive problems (flying shrapnel, angry neighbors, destroyed kitchen, etc), and probably obliterates the pickles in the process. So, the next two logical questions to ask are, "Where does behavior come from?" and "How do we find the right one for the job?"
Now, when we ask for the origins of behavior, we are really asking, "What causes behavior?" There are several answers to this depending on your frame of reference. Physiologically, behavior arises as an emergent property (epiphenomenon if you will) from the behavior of multiple neurons (and their effector organs) working together. I would be more specific if I could, be we actually have not yet identified most behaviors to particular networks of neurons. If you filled a backpack with headphones, the resulting tangled mess would give you a good analogy for the complexity of the brain. Untangling the mess is the job of neuroscientists, neuropsychologists, and basically anyone whose title starts with neuro. Behaviorists such as myself stick to the macroscopic world (but we still find the microscopic interesting), dividing our causes into two categories: proximate and ultimate. A proximate cause is the immediate antecedent to the behavior. For the behavior of answering the phone, the proximate cause is the phone ringing. The ultimate cause is more difficult to explain, but suffice it to say, determines why you behave due to a history of reinforcement. For example, you have to drive from Point A to Point B. You take route #1, but it's rush hour and it takes a long time to get there. After doing this several times, you take route #2. It is still rush hour, but you get from A to B much faster. Now the weekend comes. You take route #1 and get to point B in about the same amount of time as route #2, even though it's the same time of day. Gradually, your response is shaped to taking route #2 during rush hour and route #1 during weekends. The route you take (response) due to rush hour + time of day (cues) is a result of a history of reinforcement. If someone asked you why you took route #2 during rush hour, your response summarizes the ultimate cause (It is faster than route #1). So, the proximate cause explains why you behaved in one way as opposed to another, and the ultimate cause explains how you developed that way of behaving.
The mistake most people make when talking about behavior is dismissing the ultimate cause. When a guy in line at the coffee store yells at the person serving his coffee, you may be tempted to say, "He yelled at the worker because he is a jerk." That explains everything right? Jerks yell at people; it makes sense. Unfortunately, by doing that, you fell into B.F. Skinner's 3rd circle of Hell. Your reasoning is actually circular reasoning; he yelled at the worker because he is a jerk, and the guy is a jerk because he yelled at the worker. The ultimate cause is much less visible, having occurred in the past and over a period time, so it is very easy to miss. Additionally, the ultimate cause may be a product of evolution, further obscuring it. Widespread obesity can be attributed to physiologic mechanisms that evolved to prevent starvation (epitomized in meme form as, "Eat all the things!").
At this point, I've provided a partial explanation for the origin of behavior. Tune in next time for the epic finale.
Friday, June 29, 2012
Apparently I Have An Opinion On Health Care Too!
If you've turned on your TV, glanced at a newspaper, or checked your Facebook in the past 24 hours, you are probably aware of the US Supreme Court ruling on the PPACA (the healthcare reform signed into law back in March 2010). If you're interested in the specifics, you need only google "PPACA" or something of the sort, and you will be inundated with results about what the law entails. In super brief form, it adds several provisions designed to make sure everyone has access to healthcare, as well as means to fund these provisions. One method of funding comes from the "Individual Mandate" (IM), which requires individuals to obtain health insurance or pay a fine/penalty/tax (realistically what it's called doesn't matter because the function is the same in each case). More people buying insurance should increase competition in the market and bring down prices because those that use healthcare infrequently can help subsidize those who use it more often. The Supreme Court case was about this mandate, ultimately deciding it was constitutional under Congress's power to tax. Without the IM, the ACA would face challenges on how to fund the rest of its measures, and that would not be good.
Edit
Ran across this article just now. Should help clear up some misconceptions and disinformation.
http://www.usatoday.com/news/politics/story/2012-06-29/fact-check-court-health/55927118/1
So, why is everyone making so much noise about this law? Good question; one that has many answers. First, people are upset because they feel like they shouldn't be obligated to buy health insurance. Understandable, except for the fact that, at some point, every person will use the healthcare system. This is analogous to car insurance: if you drive a car, you are required (in nearly all states) to have insurance. That way, if someone attempts to occupy your location in space and time, you can be sure to be reimbursed for the energy the imparted into your rear bumper. If you are caught without insurance, you face a fine (sound familiar?). "But Liam," you say, "People who don't drive don't need insurance. I don't get sick, so I shouldn't need health insurance!" Unfortunately, not quite, because by virtue of being born as a human being (welcome to the club, 7 billion strong!), you have entered the healthcare market. You may never get in an accident, but you still must have insurance to cover damages. Similarly, you may never get sick, but you must have insurance to pay for services if you do. Essentially, this is designed to work like Social Security, where the old (sick) are supported by the young (healthy). Everyone becomes old at some point, so it is reasonable to collect money from everyone.
Interestingly enough, people seem to favor the provisions in the ACA, such as eliminating pre-existing conditions, but are against the IM and the law as a whole. This sort of amounts to, "we like the benefits, just not the part where we have to pay for it." While an unpleasant realization, there is no avoiding it. Healthcare is really expensive, and it shows no signs of getting cheaper spontaneously. Resources are limited, and if we don't allocate them responsibly, everyone gets screwed. The real trick is figuring out how to cut costs and manage resources while still getting quality healthcare. Originally, the focus was on waste and inefficiency in administrative and clinical settings. EHRs, streamlined billing, new payment models, and evidenced-based medicine can save money by preventing treatments and procedures that have no benefit as well as minimizing overhead costs. However, new estimates suggest that fixing 'waste' won't make up for the increasing expenditures. This doesn't mean we'll ignore all those savings; we just need to make additional changes.
Additional cuts will come from limiting some services. We will have to start saying no to some procedures and devices in some patients. Expensive imaging studies or surgical procedures may be foregone in favor of clinical diagnoses and alternative therapies. In addition, the new focus will be on preventing chronic diseases rather than attempting to manage existing ones. For example, look at diabetes and heart disease (co-morbidities in many cases too). Diabetes alone was estimated by the ADA to cost us $174 billion (in 2007). Heart disease (which includes HTN, CAD, CVA, and CHF) was estimated to cost us $272 billion (in 2010). Both diseases are highly preventable with lifestyle modifications and supportive drug therapy if necessary.
I suppose my overall point, and I'm not alone in this, is that healthcare reform is necessary and will occur no matter what goes on in government. I think that having the PPACA and IM is an important step in the right direction, but it is only the beginning. Buckle up, because there's a long, tough road ahead.
Edit
Ran across this article just now. Should help clear up some misconceptions and disinformation.
http://www.usatoday.com/news/politics/story/2012-06-29/fact-check-court-health/55927118/1
Citations
Diabetes stats: http://www.diabetes.org/diabetes-basics/diabetes-statistics/
CVD stats: http://www.theheart.org/article/1176761.do
Bloche MG. Beyond the “R Word”? Medicine's new frugality. N Engl J Med. 2012;366:1951-1953.
Blumenthal D. Performance improvement in health care — Seizing the moment. N Engl J Med. 2012;366:1953-1955.
Brody H. From an ethics of rationing to an ethics of waste avoidance. N Engl J Med. 2012;366:1949-1951.
Fuchs VR. Major trends in the U.S. health economy since 1950. N Engl J Med. 2012;366:973-977.
Song Z, Landon BE. Controlling health care spending — The Massachusetts experiment. N Engl J Med. 2012;366:1560-1561.
Thursday, June 21, 2012
Know the Difference: Allergy vs Adverse Reaction
A common question, asked at least once at every assessment. It is an important question because it is the difference between taking a drug and getting better, or say, going into anaphylactic shock. Typically, we try to avoid the latter.
2. Levinson W. Chapter 65. Hypersensitivity (Allergy). In: Levinson W, ed. Review of Medical Microbiology and Immunology. 11th ed. New York: McGraw-Hill; 2010. http://www.accessmedicine.com/content.aspx?aID=6459867. Accessed June 21, 2012.
3. Papaliodis D, Boucher W, Kempuraj D, Michaelian M, Wolfberg A, House M, Theoharide TC. Niacin-induced "flush" involves release of prostaglandin D2 from mast cells and serotonin from platelets: Evidence from human cells in vitro and an animal model. J Pharmacol Exp Ther. 2008;327:665-672.
However, the responses I've heard to this question indicate to me that there is a crucial misunderstanding about what an allergy is. On several occasions I've heard people say they are allergic to a drug, and when asked what reaction occurred, they respond with nausea or something of the sort. Of course, nausea can be a symptom of an allergic reaction, particularly in anaphylaxis. Usually though, nausea is a side effect of a medication, which is separate from an allergy. Now, time for some science and jargon!
An allergic reaction (Type I Hypersensitivity for those of you so inclined) occurs when IgE, a type of immunoglobulin (antibody), interacts with an allergen. IgE bound to the allergen can then bind to receptors on mast cells, basophils, and eosinophils to stimulate an allergic reaction. Mast cells in particular release large quantities of histamine (along with cytokines and other chemicals), which causes vasodilation as part of the inflammatory response. When vasodilation of the blood vessels in the skin occurs, the affected area will turn redder in color (also know as rubor). Other inflammatory agents like leukotrienes, cytokines, and prostaglandins contribute to the inflammatory response, causing further vasodilation, pain, and broncoconstriction. Usually the allergic reaction is limited to the immediate area where the allergen made contact. Anaphylaxis is a severe, systemic allergic response, involving broncoconstriction and global vasodilation, which leads to difficulty breathing and shock. Anaphylaxis is a life-threatening emergency, but is treatable with prompt intervention. The allergic response to a drug may occur in several different ways (Type I, II, or III), and the signs and symptoms will vary depending on the mechanism and severity. Rash and itchiness are the most common presentations of a drug allergy.
The reason allergic reactions should not be confused with side effects is because of the outcome. An allergic reaction to a drug can be very dangerous, so it is important to avoid it by using alternative medications. Side effects are often unpleasant, but rarely immediately life-threatening. For instance, the flushing that occurs when taking niacin is not an immune hypersensitivity reaction, even though it appears as one. Opioids like hydrocodone or oxycodone may cause nausea, but not due to an allergic response. Additionally, almost all medications have side effects, so it is harder to pick and choose in that case. This is why healthcare workers ask for the reaction associated with an allergy; they are trying to distinguish a true allergy from an unpleasant side effect.
I have two points, one for healthcare professionals and one for the general public. First, if you are asking a patient about any drug allergies, be sure to ask for the type of reaction that occurs. It is reasonable that the average individual may not know the difference between a side affect and allergy, but the RN/MD/DO/PA/NP needs to know whether there are any contraindications to particular medications. Second, if you are telling a healthcare worker about an adverse drug reaction, be sure to mention what happens when you take it. Additionally, if you are unsure about whether or not you are allergic to a medication, be sure to ask (and write down the response for that matter).
Sources
1. Drug allergies. PubMed Health. 2010. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001822/. Accessed June 21, 2012.
2. Levinson W. Chapter 65. Hypersensitivity (Allergy). In: Levinson W, ed. Review of Medical Microbiology and Immunology. 11th ed. New York: McGraw-Hill; 2010. http://www.accessmedicine.com/content.aspx?aID=6459867. Accessed June 21, 2012.
3. Papaliodis D, Boucher W, Kempuraj D, Michaelian M, Wolfberg A, House M, Theoharide TC. Niacin-induced "flush" involves release of prostaglandin D2 from mast cells and serotonin from platelets: Evidence from human cells in vitro and an animal model. J Pharmacol Exp Ther. 2008;327:665-672.
Sunday, June 17, 2012
In the Hospital: The Good, the Bad, and the Ugly
Ask any healthcare worker if they have interesting stories from their job, and you will be bountifully rewarded. This is especially true if said person works in an emergency department or hospital. The main reason for this effect is relatively simple: the more people you interact with, the crazier the world seems. The ED is a melting pot, with people of all demographics (though predominantly low SES) represented. Bringing such a diverse group together tends to give you interesting results.
The Ugly
ED stands for "Emergency Department," but it could also just as easily stand for "Elected to Display." What I mean by this is, people often have no shame in showing you exactly what ails them. As a volunteer, one of my jobs was to help people fill out a form so they could be triaged. We had several signs pointing to the forms, indicating they should be filled out first, but people often walked up to the window anyways. The conversation usually goes like this:
Me: Can I help you?
Patient: I need to be seen. I have this huge rash (reaches for shirt).
Me: (Quickly) Ok, I need y...
Patient: (Pulls up shirt revealing a large rash, fully in view of everyone in the room.)
Me: (To myself) Thanks for that.
Me: Ok, please fill out that form for me and we'll get you looked at. Sigh...
The probability of me being shown an ailment is proportional to how bad/disgusting it looks. If blood is involved, the chance jumps to 100%. Traumatic wounds need to be checked of course, so I don't fault people for that. It's the absurdity that gets me. You would not say, show your bulging abscess at a dinner party as part of your introduction (if it comes up in conversation, well, that's fair game). But in an ED, you'll walk up, lift your shirt triumphantly, and share with myself and others your pathological achievement.
The other common presentation is the "waited too long" patient. A couple of instances stand out in my mind. One was a woman who was extremely lethargic. She could barely even speak or hold her posture while sitting. A history revealed that she had hypothyroidism and had either run out of medication or just didn't take it for a while. Without treatment, she surely would have fallen into a myxedema coma. I remember the nurse blatantly scolding the woman and her family for not coming in sooner. The other case involved an older man who may well have set a hospital record for highest temperature in a living person. He arrived (astoundingly) by personal vehicle, driven by his daughter. He was a bigger guy, so I called the paramedic to help get him out of the van. He gave me a ribbing for not doing it myself. After a few minutes, he came back in sweating and out of breath with the patient slumped over unconscious in a wheelchair. "He was complete dead weight" the medic said (I should have gone out to help him, which I apologized for afterwards). I don't know how in hell his family got him into the car. The nurse took his temperature, which read 106.7 F (41.5 C). For those of you wondering, this is borderline "incompatible with life." The nurse wasn't even sure if the thermometer would be able to read that high. I'm fairly certain he was septic, although I think he ended up surviving. The ED really alternates between the mundane and the unbelievable.
The Bad
I'll end on good so as not to leave you feeling (too) depressed. Unfortunately, the ED is not generally a happy place. It is visited out of necessity rather than desire, which makes it ripe for unpleasantness. When you add pain/nausea/malaise/uncertainty with long, seemingly arbitrary waiting times, things can get really, really unpleasant. The worst cases occur when someone gets to "cut in line." Triage works like this: the nurse takes your vital signs and a brief history. He/She makes any quick assessments necessary, like a vision test or brief neuro exam, along with a self-reported level of pain. This is all summed up by a triage score 1-5, 1 indicating immediate life-threatening condition (like cardiac arrest) and 5 indicating minor condition with no necessary procedures (like a cold). The severity of the condition dictates who sees the doctor first. Things possibly affecting the heart (chest pain) or lungs (dyspnea) are the more common sources of line-cutting. On certain occasions, it's very obvious someone needs to go back right away (serious laceration, head trauma, altered mental status, etc) for instance, like the man who seized while being triaged. These types of problems draw few objections from the waiting room. Most times it is less obvious why someone goes back first though. One day in particular, I had a women who was fairly sick, with nausea and vomiting (n/v). However, her vitals were essentially normal, with perhaps a mild fever and and tachycardia due to the nausea. Unfortunately for her, several ambulances showed up, and we were already full. Additionally, a few other walk-ins had deviations in vital signs like hypotension, which needed to be worked up. She waited for at least three hours before she had enough. I tried to explain to her why other people went back first, but I wasn't getting through. I think she ended up leaving to go to another hospital (where she will probably wait just as long again).
On my final day, a woman showed up, depressed and on the verge of tears. She was looking for her son, who had gone missing the night before. His car was deserted, and his wallet was left behind, suspicious for foul play. But he wasn't at our hospital, and there was nothing I could do. I told the woman he wasn't at our hospital, but I would look out for the name. She then asked me what she should do. I told her to contact the police (which was her best option). She said okay, and thanked me sadly before leaving. It is a difficult thing in medicine, to want to help others but accept that sometimes, there just isn't anything you can do.
Another part of the ED is that bad news often arrives unexpectedly. People go from alive to dead without any warning or preparation. I've seen a few people coded, and not one of them survived. Listening as the doctors break the bad news is not something you easily forget. I arrived a couple times to deceased children, which is about the worst. I've seen several repeat patients, one of whom always arrives by ambulance, always complains of dyspnea, and then immediately proceeds to go outside and smoke a cigarette. Patients are often obese, some are drug seekers, some malingering for disability or other reasons. And many lack the capacity to understand how medicine and the ED works. They struggle with their own problems, and fail to appreciate the perspectives of the people trying to help them. I've seen people arrive intoxicated or high on drugs, sometimes dangerously so. Patients are combative or abusive to the staff, especially the behavioral or law enforcement ones. And the worst part of all is that so many of these people will return with the same problems, lacking the money or reinforcement they need to change. To see the human condition so exposed, so gritty, it can turn even the most optimistic people cynical.
The Good
Like most jobs that deal with the seedy side of life, you survive for the few good things. Occasionally, you will get a patient who is helpful and courteous, and it makes all the difference. Elderly people tend to be better mannered and more likely to wait patiently, but that's not always the case. The clinical and support staff can also make a big difference. Some people are naturally easy going and funny while others crumple under stress. There was one nurse in particular that I remember, because initially I think she didn't like me. When you start volunteering, you're basically a massive tool because you don't know anyone, you don't know where anything is, and you don't know how things run. As Samuel Shem puts it in the House of God, "Show me a [medical student] that only triples my work and I will kiss his feet." Such was the case with this nurse. But after spending time in triage with her, she eventually considered me a colleague/friend. If you establish yourself as a competent, trustworthy person, you'll make friends easily.
Getting to know the patients also helps. Towards the end of my volunteering career, I started spending more time talking to people. I wish I had done this sooner, because it gives you new perspectives. One man I talked to lived in NYC with his girlfriend until they broke up. He moved to a small town in Arizona, but left because of a drug problem (in the town, not necessarily himself). Another man I talked to was younger than me and had just been released from jail just a few days ago. He suffered from substance abuse and was probably in withdrawal. I chatted with him in the waiting room, and then I checked up on him once he was in a room. He was very grateful that I had spoke with him. The epitome of grateful patients occurred when a woman walked in with questions about medications for a surgery she had a few days ago (yes, she showed me the scar). I didn't want to make her wait in the ED, so I talked to the unit clerk, who managed to contact the surgeon. He said she didn't need any prescriptions for antibiotics or pain pills. I walked back out to the waiting room, expecting to hear objections raised. When I relayed the message however, she smiled and thanked me. She didn't want to take anything in the first place!
Most of my memories from the hospital are snapshots, brief clips that struck me as poignant or odd. Most are relatively neutral, but several fall under the Bad category and even fewer into Good. I learned a lot from my two and a half years at the hospital. Most importantly, I learned that communication is everything. It can mean the difference between making friends or creating enemies; the difference between gaining patient's trust or losing all credibility. What you say can make just as big an impact as what you do, medical or otherwise. When you understand a patient's perspective, it allows you to better help him or her. Medicine is all about the good, the bad, and the ugly. You just never know what your next patient is going to show you.
The Ugly
ED stands for "Emergency Department," but it could also just as easily stand for "Elected to Display." What I mean by this is, people often have no shame in showing you exactly what ails them. As a volunteer, one of my jobs was to help people fill out a form so they could be triaged. We had several signs pointing to the forms, indicating they should be filled out first, but people often walked up to the window anyways. The conversation usually goes like this:
Me: Can I help you?
Patient: I need to be seen. I have this huge rash (reaches for shirt).
Me: (Quickly) Ok, I need y...
Patient: (Pulls up shirt revealing a large rash, fully in view of everyone in the room.)
Me: (To myself) Thanks for that.
Me: Ok, please fill out that form for me and we'll get you looked at. Sigh...
The probability of me being shown an ailment is proportional to how bad/disgusting it looks. If blood is involved, the chance jumps to 100%. Traumatic wounds need to be checked of course, so I don't fault people for that. It's the absurdity that gets me. You would not say, show your bulging abscess at a dinner party as part of your introduction (if it comes up in conversation, well, that's fair game). But in an ED, you'll walk up, lift your shirt triumphantly, and share with myself and others your pathological achievement.
The other common presentation is the "waited too long" patient. A couple of instances stand out in my mind. One was a woman who was extremely lethargic. She could barely even speak or hold her posture while sitting. A history revealed that she had hypothyroidism and had either run out of medication or just didn't take it for a while. Without treatment, she surely would have fallen into a myxedema coma. I remember the nurse blatantly scolding the woman and her family for not coming in sooner. The other case involved an older man who may well have set a hospital record for highest temperature in a living person. He arrived (astoundingly) by personal vehicle, driven by his daughter. He was a bigger guy, so I called the paramedic to help get him out of the van. He gave me a ribbing for not doing it myself. After a few minutes, he came back in sweating and out of breath with the patient slumped over unconscious in a wheelchair. "He was complete dead weight" the medic said (I should have gone out to help him, which I apologized for afterwards). I don't know how in hell his family got him into the car. The nurse took his temperature, which read 106.7 F (41.5 C). For those of you wondering, this is borderline "incompatible with life." The nurse wasn't even sure if the thermometer would be able to read that high. I'm fairly certain he was septic, although I think he ended up surviving. The ED really alternates between the mundane and the unbelievable.
The Bad
I'll end on good so as not to leave you feeling (too) depressed. Unfortunately, the ED is not generally a happy place. It is visited out of necessity rather than desire, which makes it ripe for unpleasantness. When you add pain/nausea/malaise/uncertainty with long, seemingly arbitrary waiting times, things can get really, really unpleasant. The worst cases occur when someone gets to "cut in line." Triage works like this: the nurse takes your vital signs and a brief history. He/She makes any quick assessments necessary, like a vision test or brief neuro exam, along with a self-reported level of pain. This is all summed up by a triage score 1-5, 1 indicating immediate life-threatening condition (like cardiac arrest) and 5 indicating minor condition with no necessary procedures (like a cold). The severity of the condition dictates who sees the doctor first. Things possibly affecting the heart (chest pain) or lungs (dyspnea) are the more common sources of line-cutting. On certain occasions, it's very obvious someone needs to go back right away (serious laceration, head trauma, altered mental status, etc) for instance, like the man who seized while being triaged. These types of problems draw few objections from the waiting room. Most times it is less obvious why someone goes back first though. One day in particular, I had a women who was fairly sick, with nausea and vomiting (n/v). However, her vitals were essentially normal, with perhaps a mild fever and and tachycardia due to the nausea. Unfortunately for her, several ambulances showed up, and we were already full. Additionally, a few other walk-ins had deviations in vital signs like hypotension, which needed to be worked up. She waited for at least three hours before she had enough. I tried to explain to her why other people went back first, but I wasn't getting through. I think she ended up leaving to go to another hospital (where she will probably wait just as long again).
On my final day, a woman showed up, depressed and on the verge of tears. She was looking for her son, who had gone missing the night before. His car was deserted, and his wallet was left behind, suspicious for foul play. But he wasn't at our hospital, and there was nothing I could do. I told the woman he wasn't at our hospital, but I would look out for the name. She then asked me what she should do. I told her to contact the police (which was her best option). She said okay, and thanked me sadly before leaving. It is a difficult thing in medicine, to want to help others but accept that sometimes, there just isn't anything you can do.
Another part of the ED is that bad news often arrives unexpectedly. People go from alive to dead without any warning or preparation. I've seen a few people coded, and not one of them survived. Listening as the doctors break the bad news is not something you easily forget. I arrived a couple times to deceased children, which is about the worst. I've seen several repeat patients, one of whom always arrives by ambulance, always complains of dyspnea, and then immediately proceeds to go outside and smoke a cigarette. Patients are often obese, some are drug seekers, some malingering for disability or other reasons. And many lack the capacity to understand how medicine and the ED works. They struggle with their own problems, and fail to appreciate the perspectives of the people trying to help them. I've seen people arrive intoxicated or high on drugs, sometimes dangerously so. Patients are combative or abusive to the staff, especially the behavioral or law enforcement ones. And the worst part of all is that so many of these people will return with the same problems, lacking the money or reinforcement they need to change. To see the human condition so exposed, so gritty, it can turn even the most optimistic people cynical.
The Good
Like most jobs that deal with the seedy side of life, you survive for the few good things. Occasionally, you will get a patient who is helpful and courteous, and it makes all the difference. Elderly people tend to be better mannered and more likely to wait patiently, but that's not always the case. The clinical and support staff can also make a big difference. Some people are naturally easy going and funny while others crumple under stress. There was one nurse in particular that I remember, because initially I think she didn't like me. When you start volunteering, you're basically a massive tool because you don't know anyone, you don't know where anything is, and you don't know how things run. As Samuel Shem puts it in the House of God, "Show me a [medical student] that only triples my work and I will kiss his feet." Such was the case with this nurse. But after spending time in triage with her, she eventually considered me a colleague/friend. If you establish yourself as a competent, trustworthy person, you'll make friends easily.
Getting to know the patients also helps. Towards the end of my volunteering career, I started spending more time talking to people. I wish I had done this sooner, because it gives you new perspectives. One man I talked to lived in NYC with his girlfriend until they broke up. He moved to a small town in Arizona, but left because of a drug problem (in the town, not necessarily himself). Another man I talked to was younger than me and had just been released from jail just a few days ago. He suffered from substance abuse and was probably in withdrawal. I chatted with him in the waiting room, and then I checked up on him once he was in a room. He was very grateful that I had spoke with him. The epitome of grateful patients occurred when a woman walked in with questions about medications for a surgery she had a few days ago (yes, she showed me the scar). I didn't want to make her wait in the ED, so I talked to the unit clerk, who managed to contact the surgeon. He said she didn't need any prescriptions for antibiotics or pain pills. I walked back out to the waiting room, expecting to hear objections raised. When I relayed the message however, she smiled and thanked me. She didn't want to take anything in the first place!
Most of my memories from the hospital are snapshots, brief clips that struck me as poignant or odd. Most are relatively neutral, but several fall under the Bad category and even fewer into Good. I learned a lot from my two and a half years at the hospital. Most importantly, I learned that communication is everything. It can mean the difference between making friends or creating enemies; the difference between gaining patient's trust or losing all credibility. What you say can make just as big an impact as what you do, medical or otherwise. When you understand a patient's perspective, it allows you to better help him or her. Medicine is all about the good, the bad, and the ugly. You just never know what your next patient is going to show you.
Thursday, May 31, 2012
Of Schools and Secondaries
Welcome back! This is the second installment of "Liam's Somewhat Handy Guide to Applying to Medical School," and it's going to be a good one. In the first installment, we covered the Primary Application, introduced a couple tips, and tried to keep stress to a reasonable level. In this post, I'll be covering a short bit about how to decide to which schools to apply, and what the secondary applications entail (spoiler warning: money, essays, and waiting). So, let's get started.
Now, some of you might be thinking, "Liam, why did you choose to mention the schools here instead of in your post on the primary application?" A very valid question, and one I will politely choose to ignore. With that out of the way, let's talk about schools. There are 137 accredited U.S. medical schools and 17 Canadian medical schools recognized by the AAMC. The number of schools you can apply to through AMCAS differs slightly, because most Texas schools use a separate application service (TMDSAS) and some schools have multiple campuses (the University of Arizona has two campuses currently, although they're working on separate accreditation). In any case, you have about 125 choices if you plan to stay in the 50 states, and I would plan on choosing around 15-20. Why? Because of our arch nemesis, probability. Medical schools tend to follow the rule of 10%, where 10% of applicants receive an interview, and 10% of interviewees receive an acceptance (in reality, the probability of being selected after an interview is a little higher, around 15-20%, but the Rule of 10% sounds nicer). What this means is that around 1-2% of applicants to any given school actually matriculate in the fall. Now, before you reach for that bottle of whiskey, Tip #5 says "Don't Panic!" and you should strongly consider this one. Sure, the odds aren't great (still more likely than winning the lottery though). But that's why you're here looking up tips for how to improve those odds. Applying to several schools will help your chances, but you also need to make each choice count. 100 crappy applications won't beat 1 good one. Even if you're Johnny Awesomesauce, the Super Applicant.
So, now that you're completely discouraged, let's focus on how to choose specific schools. The first step is to find a copy of the MSAR®. This is your application bible. It has information on each school, including stats like average GPA and MCAT, and it can help you quickly eliminate schools that don't fit your profile. If you're as neurotic as I am, you might even enter this information into a spreadsheet to compare schools faster. I even computed Z scores for GPA and MCAT, and then averaged those to figure out how schools compared to my stats (borderline unhealthy behavior in retrospect). In any case, it'll help you eliminate schools that don't take very many OOS (out-of-state) applicants or ones where you are outside the range they usually accept. That way you don't waste time on money on an application that is doomed from the start.
The actual distribution of the 15-20 depends on you. For the love of all things holy, apply to your state school. It's almost always less expensive, and sometimes you will get some favoritism. Even if you don't intend to go there, include it. The rest of your schools should include some safety and reach choices, but make sure all your choices are places you can see yourself going to. Also, as a little note, there is a small area bias for residency locations (allegedly). What I mean is that applicants to residencies in the northeast may fare slightly better if they went to the school in the northeast. I suspect this is mostly due to familiarity and connections you develop within your area, so don't stress about this too much.
Now, this may come as a surprise to you, but medical school is basically the same everywhere. Each school has its own take on the curriculum and clinical sites, and some schools may be more focused into areas like primary care or research than others, but for the most part, they're all pretty equal. After all, an MD is an MD (it's your residency that really matters, but that comes later). My point is, don't think you have to go to a Harvard or Yale just because it's a good school. Go somewhere where you can enjoy yourself, develop new experiences, and make the most of your education. You're going to be stuck there for at least 4 years, so you damn well better choose a place where you can be happy. And, since we haven't introduced a new tip in a while, here's one now:
Tip #7: Be passionate.
Really, this should extend in to all aspects of your life. If you don't find yourself passionate or excited about the school, it's probably not the one for you (hint, you can substitute person for school to apply this to relationships too). People generally do better work when they are happy and motivated (or at least they don't mind the work as much), so it makes sense to maximize your chances of being in a positive frame of mind.
Secondaries
I've just gone on and on and on about choosing a school, and I've only barely mentioned the secondary application. There's a reason for this (Spoiler alert!). The secondary is really just a couple more essays, on average, I would guess about three, with a ludicrous fee. One essay is usually a "Why do you want to go here?" type, which is fairly self-explanatory. Look up information about the school, and talk about how it matches your experiences and goals. Check, one down. Another essay I encountered frequently asked, "How would you contribute to the diversity of the student body?" (ie what makes you unique?). This one can be tricky. It is really up to you to decide what aspect of your personality and history you focus on. If you're really struggling like I was, ask your friends and family for help. Sometimes you can overlook an event or behavior that's worth talking about. Those two are the ones that appear frequently. Keep in mind secondaries are pretty heterogeneous. Some had no essays (awesome, except for the money part) and a couple had 7+ essays (rarely, thank god). SDN has school-specific threads for the current cycle and previous one, so you can often check past threads to see how many and what type of questions the last group had.
Otherwise, there's not much to it. This is where the long waits come in. Most schools send secondaries to everyone, so the earliest you receive yours is usually based on when they received your primary. When you do get it, try to fill it out in a reasonable amount of time. That way, if you're filling out multiple secondaries, you don't get too bogged down. I would also recommend having all secondaries submitted and complete (LORs received) by the end of August. Interviews start around September, and you want to give yourself as much time as possible to be selected. After you submit your secondary, try not to obsess over it. The wait will be long and stressful, but if you keep checking SDN to see who is getting interviews, it will be that much longer and more stressful. But that's it. And not only that, most of the hard work is done! You still have the interview, but your chances greatly improve if you can get that invitation. So, put away the Tums for now and go enjoy your summer. If you have to wait, may as well make the most of it!
Now, some of you might be thinking, "Liam, why did you choose to mention the schools here instead of in your post on the primary application?" A very valid question, and one I will politely choose to ignore. With that out of the way, let's talk about schools. There are 137 accredited U.S. medical schools and 17 Canadian medical schools recognized by the AAMC. The number of schools you can apply to through AMCAS differs slightly, because most Texas schools use a separate application service (TMDSAS) and some schools have multiple campuses (the University of Arizona has two campuses currently, although they're working on separate accreditation). In any case, you have about 125 choices if you plan to stay in the 50 states, and I would plan on choosing around 15-20. Why? Because of our arch nemesis, probability. Medical schools tend to follow the rule of 10%, where 10% of applicants receive an interview, and 10% of interviewees receive an acceptance (in reality, the probability of being selected after an interview is a little higher, around 15-20%, but the Rule of 10% sounds nicer). What this means is that around 1-2% of applicants to any given school actually matriculate in the fall. Now, before you reach for that bottle of whiskey, Tip #5 says "Don't Panic!" and you should strongly consider this one. Sure, the odds aren't great (still more likely than winning the lottery though). But that's why you're here looking up tips for how to improve those odds. Applying to several schools will help your chances, but you also need to make each choice count. 100 crappy applications won't beat 1 good one. Even if you're Johnny Awesomesauce, the Super Applicant.
So, now that you're completely discouraged, let's focus on how to choose specific schools. The first step is to find a copy of the MSAR®. This is your application bible. It has information on each school, including stats like average GPA and MCAT, and it can help you quickly eliminate schools that don't fit your profile. If you're as neurotic as I am, you might even enter this information into a spreadsheet to compare schools faster. I even computed Z scores for GPA and MCAT, and then averaged those to figure out how schools compared to my stats (borderline unhealthy behavior in retrospect). In any case, it'll help you eliminate schools that don't take very many OOS (out-of-state) applicants or ones where you are outside the range they usually accept. That way you don't waste time on money on an application that is doomed from the start.
The actual distribution of the 15-20 depends on you. For the love of all things holy, apply to your state school. It's almost always less expensive, and sometimes you will get some favoritism. Even if you don't intend to go there, include it. The rest of your schools should include some safety and reach choices, but make sure all your choices are places you can see yourself going to. Also, as a little note, there is a small area bias for residency locations (allegedly). What I mean is that applicants to residencies in the northeast may fare slightly better if they went to the school in the northeast. I suspect this is mostly due to familiarity and connections you develop within your area, so don't stress about this too much.
Now, this may come as a surprise to you, but medical school is basically the same everywhere. Each school has its own take on the curriculum and clinical sites, and some schools may be more focused into areas like primary care or research than others, but for the most part, they're all pretty equal. After all, an MD is an MD (it's your residency that really matters, but that comes later). My point is, don't think you have to go to a Harvard or Yale just because it's a good school. Go somewhere where you can enjoy yourself, develop new experiences, and make the most of your education. You're going to be stuck there for at least 4 years, so you damn well better choose a place where you can be happy. And, since we haven't introduced a new tip in a while, here's one now:
Tip #7: Be passionate.
Really, this should extend in to all aspects of your life. If you don't find yourself passionate or excited about the school, it's probably not the one for you (hint, you can substitute person for school to apply this to relationships too). People generally do better work when they are happy and motivated (or at least they don't mind the work as much), so it makes sense to maximize your chances of being in a positive frame of mind.
Secondaries
I've just gone on and on and on about choosing a school, and I've only barely mentioned the secondary application. There's a reason for this (Spoiler alert!). The secondary is really just a couple more essays, on average, I would guess about three, with a ludicrous fee. One essay is usually a "Why do you want to go here?" type, which is fairly self-explanatory. Look up information about the school, and talk about how it matches your experiences and goals. Check, one down. Another essay I encountered frequently asked, "How would you contribute to the diversity of the student body?" (ie what makes you unique?). This one can be tricky. It is really up to you to decide what aspect of your personality and history you focus on. If you're really struggling like I was, ask your friends and family for help. Sometimes you can overlook an event or behavior that's worth talking about. Those two are the ones that appear frequently. Keep in mind secondaries are pretty heterogeneous. Some had no essays (awesome, except for the money part) and a couple had 7+ essays (rarely, thank god). SDN has school-specific threads for the current cycle and previous one, so you can often check past threads to see how many and what type of questions the last group had.
Otherwise, there's not much to it. This is where the long waits come in. Most schools send secondaries to everyone, so the earliest you receive yours is usually based on when they received your primary. When you do get it, try to fill it out in a reasonable amount of time. That way, if you're filling out multiple secondaries, you don't get too bogged down. I would also recommend having all secondaries submitted and complete (LORs received) by the end of August. Interviews start around September, and you want to give yourself as much time as possible to be selected. After you submit your secondary, try not to obsess over it. The wait will be long and stressful, but if you keep checking SDN to see who is getting interviews, it will be that much longer and more stressful. But that's it. And not only that, most of the hard work is done! You still have the interview, but your chances greatly improve if you can get that invitation. So, put away the Tums for now and go enjoy your summer. If you have to wait, may as well make the most of it!
Friday, May 11, 2012
Behavior: It's What You Do!
As far as undergraduate majors go, psychology is typically one of the more popular ones. This occurs for a variety of reasons, but I suspect the relatively easy course material plays the dominant role. Psychology has the sophisticated appearance of a science without all that pesky scientific rigor and prerequisite chemistry and biology work (not actually true). The theories and concepts put forth by people like Descartes and Freud sound very scientific and appear to explain why people act as they do. Unfortunately, Freud's theories suffer from the problem of being completely un-testable, which just doesn't fly with those who practice the scientific method. Additionally, his data came primarily from case studies, which are great for identifying problems and events that need explaining, but cannot be used as compelling empirical evidence. Despite this, pop psychology is immensely, um, popular because it uses cool words like transference and cognition and describes events we can relate to. But those are problems for another day. Instead, I am going to introduce behavior and how I was trained to view psychology from a behavioral perspective.
Behavior can be defined in several ways. So far, the most useful definition comes from a functional standpoint: A behavior is an action that solves an adaptive problem. An adaptive problem is a fancy term for some event that affects your fitness (reproductive success). For instance, say you are out for a nice evening stroll through the park. It is a pleasant night, and although you are annoyed that Tom didn't fax his request for additional copy paper before leaving for the day, you are ultimately in a good mood. As you pass by the rock formation shaped in the uncanny likeness of John Belushi, you encounter a very aggressive-looking lion. The presence of the lion (called the context, more on that later) presents you with an adaptive problem: Your fitness will decrease substantially if the lion is allowed to solve his adaptive problem (to my knowledge, there are no cases of successful reproduction when one partner is deceased. The internet may suggest otherwise). In any case, your response to the lion is a behavior. It might consist of fighting the lion, running away from the lion, bargaining with your choice of higher power, or attempting to persuade the lion that you are not a suitable source of food (what you end up doing depends on your behavioral and evolutionary history, but again, more on this later). What matters is that you were presented with a problem that would affect your fitness, and you responded in a manner to address that problem. Even mundane activities such as driving to work, checking your mail, and watching TV can be called adaptive problems, because they affect your ability to acquire/distribute resources or attract a mate. Behavior is everywhere, and you are doing it all the time.
(As a clarification, behavior is specifically what you do, never what you are not doing. Avoiding your homework is not a behavior because it fails the so called "dead-man test." If a dead person can do it, it isn't behavior) (Malott & Suarez, 2004)
There is also a special type of behavior that describes the transfer of information (essentially cues) between individuals. We, unimaginatively perhaps, call this type of behavior verbal behavior. Your speech and non-verbal communication is considered behavior because again, it solves adaptive problems (and involves a verbal episode, which is the exchange of discriminative stimuli). You might say, "Honey, please pass the salt" or "Did I tell you about the time I was attacked by a lion?" to initiate the verbal episode. The other person will respond, either continuing or concluding the episode. Verbal behavior also includes nonverbal actions like facial expressions, body language, sign language, and even ordinary signs, like those you might see on the road or warning you to wear a hard hat. Remember, if you do it, it is behavior (pending passing the dead man test).
Behavioral psychologists are usually less interested in the behavior itself, and more interested in the adaptive problems it may solve. Often times it is unclear what adaptive function a behavior serves, as in schizophrenia or depression. Sometimes the adaptive function is diminished over time or disappears entirely, but the behavior continues anyways, such as using eating utensils or consuming high-caloric foods. Luckily, the very principles that lead behavior astray can also help fix it.
Behaviorism is not a complicated subject. Many of the concepts and principles are intuitive and similar to concepts in other sciences (especially with respect to evolutionary theory). The core philosophy of behaviorism though, drastically contrasts the popular, dualistic notions of psychology, and it can be profoundly difficult to unlearn those notions. I promise however, that once you start seeing the world through behavior-colored lenses, it becomes much easier to identify problems and institute actions to fix them. After all, behavior is what you do. What could be simpler than that?
My information comes from my behavioral psych professor and these two books (both available on Amazon). If you're looking for much more detail on behaviorism and behavior, give these a read:
1. Principles of Behavior by Richard Malott and Elizabeth Suarez.
2. Understanding Behaviorism: Behavior, Culture, and Evolution by William Baum.
Behavior can be defined in several ways. So far, the most useful definition comes from a functional standpoint: A behavior is an action that solves an adaptive problem. An adaptive problem is a fancy term for some event that affects your fitness (reproductive success). For instance, say you are out for a nice evening stroll through the park. It is a pleasant night, and although you are annoyed that Tom didn't fax his request for additional copy paper before leaving for the day, you are ultimately in a good mood. As you pass by the rock formation shaped in the uncanny likeness of John Belushi, you encounter a very aggressive-looking lion. The presence of the lion (called the context, more on that later) presents you with an adaptive problem: Your fitness will decrease substantially if the lion is allowed to solve his adaptive problem (to my knowledge, there are no cases of successful reproduction when one partner is deceased. The internet may suggest otherwise). In any case, your response to the lion is a behavior. It might consist of fighting the lion, running away from the lion, bargaining with your choice of higher power, or attempting to persuade the lion that you are not a suitable source of food (what you end up doing depends on your behavioral and evolutionary history, but again, more on this later). What matters is that you were presented with a problem that would affect your fitness, and you responded in a manner to address that problem. Even mundane activities such as driving to work, checking your mail, and watching TV can be called adaptive problems, because they affect your ability to acquire/distribute resources or attract a mate. Behavior is everywhere, and you are doing it all the time.
(As a clarification, behavior is specifically what you do, never what you are not doing. Avoiding your homework is not a behavior because it fails the so called "dead-man test." If a dead person can do it, it isn't behavior) (Malott & Suarez, 2004)
There is also a special type of behavior that describes the transfer of information (essentially cues) between individuals. We, unimaginatively perhaps, call this type of behavior verbal behavior. Your speech and non-verbal communication is considered behavior because again, it solves adaptive problems (and involves a verbal episode, which is the exchange of discriminative stimuli). You might say, "Honey, please pass the salt" or "Did I tell you about the time I was attacked by a lion?" to initiate the verbal episode. The other person will respond, either continuing or concluding the episode. Verbal behavior also includes nonverbal actions like facial expressions, body language, sign language, and even ordinary signs, like those you might see on the road or warning you to wear a hard hat. Remember, if you do it, it is behavior (pending passing the dead man test).
Behavioral psychologists are usually less interested in the behavior itself, and more interested in the adaptive problems it may solve. Often times it is unclear what adaptive function a behavior serves, as in schizophrenia or depression. Sometimes the adaptive function is diminished over time or disappears entirely, but the behavior continues anyways, such as using eating utensils or consuming high-caloric foods. Luckily, the very principles that lead behavior astray can also help fix it.
Behaviorism is not a complicated subject. Many of the concepts and principles are intuitive and similar to concepts in other sciences (especially with respect to evolutionary theory). The core philosophy of behaviorism though, drastically contrasts the popular, dualistic notions of psychology, and it can be profoundly difficult to unlearn those notions. I promise however, that once you start seeing the world through behavior-colored lenses, it becomes much easier to identify problems and institute actions to fix them. After all, behavior is what you do. What could be simpler than that?
My information comes from my behavioral psych professor and these two books (both available on Amazon). If you're looking for much more detail on behaviorism and behavior, give these a read:
1. Principles of Behavior by Richard Malott and Elizabeth Suarez.
2. Understanding Behaviorism: Behavior, Culture, and Evolution by William Baum.
Monday, May 7, 2012
In the Hospital, Day 1
One hot summer afternoon, I walked into the emergency department (ED) at a local hospital for the first time. I was nervous about my new position because at no point did I receive any substantial training. I was shown places where important items were present and should be, as well as places where important items weren't but should have been. My function was to remedy the situation so that all the places fell under the first category (this was very rarely achieved in full). I was also more or less in charge of the waiting room, which meant I would be the first person patients and visitors would address with their questions and comments. At first this seemed problematic, given the absence of training and a lack of knowledge on hospital procedures. But it quickly became clear that only a few phrases would be necessary, most of which include the words "wait" and "soon" in some configuration.
It was a small waiting room, with enough chairs for approximately twenty-five people. The triage area, nicknamed The Fishbowl, overlooked the room from the corner. The Fishbowl owed its nickname to the plexiglass windows that closed it off from the waiting room (more importantly, the people in the waiting room). Thankfully, it was not too busy, which I considered a good omen. I swiped my badge, and proceeded through the double doors that led to the rest of the hospital and the ED. There I met Roger (not his real name), the volunteer who offered to lend for my first day. His first two pieces of advice immediately contradicted the little training I was given. First, he recommended that I avoid doing "Rounds" on the people waiting. This tended to disturb the fragile equilibrium between people asking me questions and people becoming frustrated with my "wait" and "soon" responses. Once a patient views you as a foe, your job becomes infinitely more difficult and miserable, and so we decided it was best to let sleeping dogs lie (especially the people actually sleeping). Second, he recommended that I stay inside the Fishbowl. This allowed me to watch over the room and get to know the triage nurse while further discouraging questions. And so we set off, thwarting attempts to bother the nurse, helping family members find a relative, and keeping individuals contently (quietly) waiting.
Before my volunteer savior left me to manage alone, a patient arrived by EMS suffering from seizures (unknown to Roger and I). One woman was particularly hysterical, pacing back and forth, barely able to form complete sentences. She pleaded with us to let us see the patient, but he wasn't settled in yet (IVs, meds, exam, etc). At first we didn't even know who she was talking about, and before we could get any information from her, she hurried outside to make a phone call. Roger shrugged, and we went back to work. Later, I recall walking by his bed as he began seizing again. Had it not been my first day, I would have paused briefly to see how they were managing him. Eventually, the woman was let back to see him, although she was somewhat of a thorn in the side of the staff.
The rest of the evening was less eventful, but busier (which tends to be both a good thing and a bad thing). As I was leaving (an hour after my shift was supposed to end), the triage nurse, recognizing that it was my first day, gave me some advice (which I would not heed nor fully appreciate until much later). He told me, "don't forget to have fun." It's easy to spend all your time volunteering or studying or focusing so much on your goals that you forget to take a breather. I left that night tired but excited. This was my first step into the world of medicine, and it was sure to be interesting.
It was a small waiting room, with enough chairs for approximately twenty-five people. The triage area, nicknamed The Fishbowl, overlooked the room from the corner. The Fishbowl owed its nickname to the plexiglass windows that closed it off from the waiting room (more importantly, the people in the waiting room). Thankfully, it was not too busy, which I considered a good omen. I swiped my badge, and proceeded through the double doors that led to the rest of the hospital and the ED. There I met Roger (not his real name), the volunteer who offered to lend for my first day. His first two pieces of advice immediately contradicted the little training I was given. First, he recommended that I avoid doing "Rounds" on the people waiting. This tended to disturb the fragile equilibrium between people asking me questions and people becoming frustrated with my "wait" and "soon" responses. Once a patient views you as a foe, your job becomes infinitely more difficult and miserable, and so we decided it was best to let sleeping dogs lie (especially the people actually sleeping). Second, he recommended that I stay inside the Fishbowl. This allowed me to watch over the room and get to know the triage nurse while further discouraging questions. And so we set off, thwarting attempts to bother the nurse, helping family members find a relative, and keeping individuals contently (quietly) waiting.
Before my volunteer savior left me to manage alone, a patient arrived by EMS suffering from seizures (unknown to Roger and I). One woman was particularly hysterical, pacing back and forth, barely able to form complete sentences. She pleaded with us to let us see the patient, but he wasn't settled in yet (IVs, meds, exam, etc). At first we didn't even know who she was talking about, and before we could get any information from her, she hurried outside to make a phone call. Roger shrugged, and we went back to work. Later, I recall walking by his bed as he began seizing again. Had it not been my first day, I would have paused briefly to see how they were managing him. Eventually, the woman was let back to see him, although she was somewhat of a thorn in the side of the staff.
The rest of the evening was less eventful, but busier (which tends to be both a good thing and a bad thing). As I was leaving (an hour after my shift was supposed to end), the triage nurse, recognizing that it was my first day, gave me some advice (which I would not heed nor fully appreciate until much later). He told me, "don't forget to have fun." It's easy to spend all your time volunteering or studying or focusing so much on your goals that you forget to take a breather. I left that night tired but excited. This was my first step into the world of medicine, and it was sure to be interesting.
Wednesday, May 2, 2012
Applying to Medical School, the Primary
May is here again, which heralds the beginning of the 2013 admissions application cycle. Thousands of pre-medical students will begin filling out their AMCAS applications (the primary application), inputting a long list of information that seems slightly redundant. However, this should not discourage a pre-med, because by this time, hoop-jumping and tedious activities should be well practiced. Assuming you are a pre-med, let's go over some of the stuff you will need for the primary. (Note: These are my recommendations and experiences with the application. Your experience will differ. Take my advice with a healthy degree of skepticism and maybe an antacid).
Also note: This is a longer post. Use the search function to find what you're looking for, although I'd love it if you read the entire thing. I wrote all this stuff for a reason you know...
We start at the AMCAS application page. AMCAS is an acronym that is entirely unimportant; just think of it as the primary application, where grades, letters of recommendation, your relevant experiences, and the personal statement go. Eventually you will associate it with frustration, anxiety, and a vague sense of abdominal discomfort, but that comes later. Currently on the front page is a 20 minute video about the application. I suggest you watch it. Better yet, read the manual too. (A stretch I know, but suck it up. You're in for a lot of reading in medical school anyways). In fact, let's do that right now. Grab a snack, close out of Facebook, and give the video a go.
... Finished? Fantastic! That was a lot of material, and you may feel that mild abdominal discomfort developing already. Congratulations, you're ahead of the game! But like Douglas Adams said, "Don't panic." As with any large project, if you tackle it systematically, everything will turn out okay.
Coursework
As part of the application, you will have to input your coursework. This includes every class you've ever taken at a college, including community college and college credits you may have earned during high school. You will also need transcripts from each school you've attended. When you enter in your courses, you want to match the transcript as closely as possible, down to the course name and code. The manual has a couple special cases for certain classes, like combined lecture/lab classes. It is also okay to specify which semester a class is if it isn't explicit in the name (for example, if the name of organic chemistry is the same for both semesters, you can add a I and II or 1 and 2 to indicate first and second semester). Double and triple check that you entered everything correctly before you submit, as inconsistencies may hold up your application.
The rest of the application is not very complicated; there just happens to be a lot to fill out. That being said, here are the first two tips:
Tip #1: Use common sense. If you are completely unsure, ask for help.
Tip #2 : Be honest. Be yourself.
These tips extend through the entire application process really. The application is not trying to trick you. In fact, this application will be the predominant way the Adcoms (and possibly the interviewer) will get to know you. On one interview, I actually sat down with my interviewer as she went through my primary application bit by bit. So be reasonable. Answer questions as you would answer to a friend. Be completely honest, because you may end up being asked questions about your essays or personal statement.
Work/Activities
The work/activities part is where you enter information about the things you've done during college. This section and the personal statement are really the only ways the Adcoms will be able to get to know you as an individual, so do not skimp. That being said, you don't have much room, so you'll have to be concise as well. This leads into my next tip:
Tip #3: Don't sell yourself short!
You are applying to medical school. Just think about that for a second. That's pretty awesome. You've worked your ass off throughout undergraduate just to get to this moment. Sure, there's someone who set up clinics in Africa while rescuing infants from a burning building and scoring a 52Y on the MCAT. There's someone who somehow cured AIDS, cancer, and eczema with a single discovery. Don't focus on that. They're probably really boring anyways. Adcoms want people who are enthusiastic and genuine. Don't try to be something you aren't, but be proud of the things you've accomplished and what you think is important. Plus, you'll write better about things you naturally find interesting.
Personal Statement
The personal statement is similar in that regard, except it is longer and more like a story. Do not simply restate your activities. You want to demonstrate how your experiences and personality make you an excellent candidate. I took a couple of experiences I found most profound, and used them to tell a story about how they shaped my perception of medicine and the kind of doctor I wanted to be. My theme was fun; medicine is serious business but there's no reason why it can't be fun as well. So try to enjoy writing your personal statement. Imagine that J.K. Rowling wanted to write a book using you as the main character. Be memorable (in a good way. Spelling and grammar mistakes or completely inappropriate material may be 'memorable', but will probably hurt your chances). I suggest you have several people look it over too. Find an English major (better yet, creative writing) and ask him/her to make suggestions. They will be flattered that you need their skills.
Letters, schools, and miscellaneous stuff
We'll start with a tip:
Tip #4: Read everything thoroughly.
Make sure you read the instructions, questions, responses, everything completely. I'm serious. You can't change most of the application after you submit it. You'll kick yourself if you missed the "not" in a question, or used one school's essay for another one and forgot to change the names (not me thank god, but I heard stories). Minor mistakes can usually be clarified with individual schools (I messed up a course code so it looked like I listed the same course twice). For LoRs, make sure you check each school's requirements. Some cap how many they'll accept (min and max), and most specify from whom the letters should come.
Tip #5: Don't panic!
I'm saying this twice for a reason. Applying to medical school has a way of giving people ulcers (and emptying their wallets). You've spent years getting to this point. You've shadowed, volunteered, studied, tested, and worked far more hours than you've slept. Now you have to summarize those years in just a couple paragraphs, pay an absurd amount of money, and wait. Then, secondaries will come back, meaning more writing and more money. This is followed by a lot more waiting. You'll go interview, where everyone else seems to be more qualified and experienced. Then you wait some more. Eventually, mail will start arriving. Waiting and lists, two hallmarks of the application process, will be combined into one nebulous and depressing package. Rejections will test your resolve and patience. But, stay with me here, But, you'll check your email and see "Congratulations" in the heading, and promptly spend the remainder of the day getting absolutely smashed. And at no point should you panic. Mistakes can be fixed with a polite email. Your friends and other applicants can commiserate together. Even in a worst case scenario, there will be another application cycle coming around. There are many paths to medical school, and no one is best. So, don't panic. In the end, the people who get into medical school are not necessarily the ones with the highest grades or longest resume. The people who are accepted are the ones who are the most persistent and confident that they would make great doctors.
Also note: This is a longer post. Use the search function to find what you're looking for, although I'd love it if you read the entire thing. I wrote all this stuff for a reason you know...
We start at the AMCAS application page. AMCAS is an acronym that is entirely unimportant; just think of it as the primary application, where grades, letters of recommendation, your relevant experiences, and the personal statement go. Eventually you will associate it with frustration, anxiety, and a vague sense of abdominal discomfort, but that comes later. Currently on the front page is a 20 minute video about the application. I suggest you watch it. Better yet, read the manual too. (A stretch I know, but suck it up. You're in for a lot of reading in medical school anyways). In fact, let's do that right now. Grab a snack, close out of Facebook, and give the video a go.
... Finished? Fantastic! That was a lot of material, and you may feel that mild abdominal discomfort developing already. Congratulations, you're ahead of the game! But like Douglas Adams said, "Don't panic." As with any large project, if you tackle it systematically, everything will turn out okay.
Coursework
As part of the application, you will have to input your coursework. This includes every class you've ever taken at a college, including community college and college credits you may have earned during high school. You will also need transcripts from each school you've attended. When you enter in your courses, you want to match the transcript as closely as possible, down to the course name and code. The manual has a couple special cases for certain classes, like combined lecture/lab classes. It is also okay to specify which semester a class is if it isn't explicit in the name (for example, if the name of organic chemistry is the same for both semesters, you can add a I and II or 1 and 2 to indicate first and second semester). Double and triple check that you entered everything correctly before you submit, as inconsistencies may hold up your application.
The rest of the application is not very complicated; there just happens to be a lot to fill out. That being said, here are the first two tips:
Tip #1: Use common sense. If you are completely unsure, ask for help.
Tip #2 : Be honest. Be yourself.
These tips extend through the entire application process really. The application is not trying to trick you. In fact, this application will be the predominant way the Adcoms (and possibly the interviewer) will get to know you. On one interview, I actually sat down with my interviewer as she went through my primary application bit by bit. So be reasonable. Answer questions as you would answer to a friend. Be completely honest, because you may end up being asked questions about your essays or personal statement.
Work/Activities
The work/activities part is where you enter information about the things you've done during college. This section and the personal statement are really the only ways the Adcoms will be able to get to know you as an individual, so do not skimp. That being said, you don't have much room, so you'll have to be concise as well. This leads into my next tip:
Tip #3: Don't sell yourself short!
You are applying to medical school. Just think about that for a second. That's pretty awesome. You've worked your ass off throughout undergraduate just to get to this moment. Sure, there's someone who set up clinics in Africa while rescuing infants from a burning building and scoring a 52Y on the MCAT. There's someone who somehow cured AIDS, cancer, and eczema with a single discovery. Don't focus on that. They're probably really boring anyways. Adcoms want people who are enthusiastic and genuine. Don't try to be something you aren't, but be proud of the things you've accomplished and what you think is important. Plus, you'll write better about things you naturally find interesting.
Personal Statement
The personal statement is similar in that regard, except it is longer and more like a story. Do not simply restate your activities. You want to demonstrate how your experiences and personality make you an excellent candidate. I took a couple of experiences I found most profound, and used them to tell a story about how they shaped my perception of medicine and the kind of doctor I wanted to be. My theme was fun; medicine is serious business but there's no reason why it can't be fun as well. So try to enjoy writing your personal statement. Imagine that J.K. Rowling wanted to write a book using you as the main character. Be memorable (in a good way. Spelling and grammar mistakes or completely inappropriate material may be 'memorable', but will probably hurt your chances). I suggest you have several people look it over too. Find an English major (better yet, creative writing) and ask him/her to make suggestions. They will be flattered that you need their skills.
Letters, schools, and miscellaneous stuff
We'll start with a tip:
Tip #4: Read everything thoroughly.
Make sure you read the instructions, questions, responses, everything completely. I'm serious. You can't change most of the application after you submit it. You'll kick yourself if you missed the "not" in a question, or used one school's essay for another one and forgot to change the names (not me thank god, but I heard stories). Minor mistakes can usually be clarified with individual schools (I messed up a course code so it looked like I listed the same course twice). For LoRs, make sure you check each school's requirements. Some cap how many they'll accept (min and max), and most specify from whom the letters should come.
Tip #5: Don't panic!
I'm saying this twice for a reason. Applying to medical school has a way of giving people ulcers (and emptying their wallets). You've spent years getting to this point. You've shadowed, volunteered, studied, tested, and worked far more hours than you've slept. Now you have to summarize those years in just a couple paragraphs, pay an absurd amount of money, and wait. Then, secondaries will come back, meaning more writing and more money. This is followed by a lot more waiting. You'll go interview, where everyone else seems to be more qualified and experienced. Then you wait some more. Eventually, mail will start arriving. Waiting and lists, two hallmarks of the application process, will be combined into one nebulous and depressing package. Rejections will test your resolve and patience. But, stay with me here, But, you'll check your email and see "Congratulations" in the heading, and promptly spend the remainder of the day getting absolutely smashed. And at no point should you panic. Mistakes can be fixed with a polite email. Your friends and other applicants can commiserate together. Even in a worst case scenario, there will be another application cycle coming around. There are many paths to medical school, and no one is best. So, don't panic. In the end, the people who get into medical school are not necessarily the ones with the highest grades or longest resume. The people who are accepted are the ones who are the most persistent and confident that they would make great doctors.
Sunday, April 29, 2012
The Beginning
I know what you're thinking. Does the world need another blog about medical school? Have we not already exhausted the finite number of ways to describe the endless studying, the mindless scut-work, the boundless financial debt? Will my material be as repetitive and lackluster as the examples I just provided? Probably. As a traditional applicant, the journey through undergraduate, medical school, residency, and beyond follows a well-traveled path. A somewhat rocky and winding path, but highly traversed nonetheless. It is not my intention to revolutionize this journey. But I do hope to add my insight and experiences to the burgeoning collection, partially for myself, to reflect upon and organize my thoughts and beliefs, and for other students, to help them develop and navigate through their own adventures.
I am not the first to use a medical acronym in the title of my blog (not even the first to use this acronym). But I believe it accurately summarizes what I hope to accomplish. The SOAP note is a quick way to describe the management of an individual patient. Its constituent parts are Subjective (anything the patient reports), Objective (anything the physician can report), Assessment, and Plan. And so I plan (I'll hit each one, don't you worry) to populate this blog with my own musings and anecdotes on matters that are relevant to myself, other students, no one in particular, or no one at all. Whether they are experiences with people or the idiosyncrasies of medical education, I hope to infuse humor when appropriate (and a little bit less humor when wholly inappropriate) to make each story enjoyable, or at a very minimum, tolerable. Periodically, I also plan on including interesting scientific information or facts pertaining to the study of medicine, from pre-medical to post-graduate. And because I hail from a behaviorist research lab, I will sneak tidbits of behaviorism and psychology when I can. Humor will accompany these facts and theories, although it will be of the dry variety and quite possibly not funny to anyone other than myself and those who assume Fargo is a comedy. Now the assessment is trickier. It will tend to show up when I am trying to make a point or provide a moral to a story.
And so we come back to plan. As I await the beginning of medical school, my plan is to provide a review of the application process, as well as spend some time recounting a few of my more substantial pre-medical experiences. Once August rolls around, all bets are off.
-Liam
Note: In the event it appears this blog appears abandoned, enjoy the content I managed to provide.
Note: In the event the blog is abandoned because I was murdered under suspicious circumstances, I can assure you there is no hidden message present. Also, please enjoy the content I managed to provide.
And so we come back to plan. As I await the beginning of medical school, my plan is to provide a review of the application process, as well as spend some time recounting a few of my more substantial pre-medical experiences. Once August rolls around, all bets are off.
-Liam
Note: In the event it appears this blog appears abandoned, enjoy the content I managed to provide.
Note: In the event the blog is abandoned because I was murdered under suspicious circumstances, I can assure you there is no hidden message present. Also, please enjoy the content I managed to provide.
Subscribe to:
Comments (Atom)