Overall, medical school is pretty great. At least that's what I keep telling myself. The workload is insane, your world gets reduced to things in and around med school, the debt is.. well we just won't even go there. But it's a worthwhile endeavor, and you tend to feel accomplished when you pass your exams or impress your clinical leaders. And you're surrounded by 100+ people all doing the same thing, so there's a sense of camaraderie (the people in our class are pretty awesome).
However, I do have one criticism, one qualm if you will, about medical school, and it is this: you constantly feel like you're being thrown from one thing to the next. Unfortunately, I don't really see any alternative. Originally I planned on writing about how the layout and culture of medical education promote this shuttling behavior, and how it hurts students in both the short term and long term. After thinking about it though, I don't really see what could be different. Medical school year one is a strange place. The first semester, you barrel through biochem and anatomy while starting your intro to medicine and problem based learning classes. The sciences are particularly guilty of moving from topic to topic. Granted, they have a lot of material to cover. Unfortunately, you almost constantly feel that by the time you master something, you have two or three new things to do (if you're lucky, only two or three things).
Additionally, you're often shuttled from one topic you've never encountered before to another topic you've never encountered before. The intro medicine class is very guilty of this. For example, we interviewed our first real patients as part of the class. We did this without really knowing what we were supposed to accomplish or even how to do it. And this really gets to the root of my criticism. I think the reason we (fine, I) feel like we're bouncing along from one thing to the other is simply because there's an abundance of information, and we haven't yet developed the filters to manage it yet. It's difficult to know what the important parts of biochem and anatomy are because we haven't had an exam to spotlight where the important details are coming from. Intro to medicine is even worse because we have almost zero knowledge about which questions are important and relevant. So, even when we know what to ask, we have no idea why we're doing it. And strangely enough, we won't even get that knowledge until second year, when pathophysiology is discussed.
But, I can see why we do it this way. First, curricula are hard to completely reinvent so we can only reform parts at a time. Plus people dislike change; blame it on the humans. Second, you can't filter information if you don't have any to start with. If I don't learn how to take a detailed history, I won't know which parts I can skip over or include. If I don't memorize the muscles and there innervations, I won't have the information to make a diagnosis. If I don't know how the cell membrane is affected by deviations in extracellular potassium... well, that one is stretching it. Ultimately, we just have to run the gauntlet and assume/tell ourselves it will work out in the end.
Thursday, September 6, 2012
Monday, August 27, 2012
What Beautiful Anatomy You Have
Med school marches onward, seemingly oblivious to the poor souls it's dragging with it. Realistically, we are a boiler, gradually building up pressure until that first exam hits and we burst out the safety release valve. That will be an interesting day for sure.
This week was notable for our first anatomy dissection. Every med school I know of has a cadaver dissection as part of the course, the point being to help us learn anatomy. To say it is an odd experience is downplaying it rather substantially. For one, death is not a topic that is addressed in casual conversation, thus evoking some anxious feelings when it is presented in such an explicit form. Additionally, cutting apart the flesh of the deceased is surreal. Generally, we tend to discourage stabbing other humans with scalpels and scissors and other pointy objects. Making cuts into the body requires you to fight back against decades of rule governed behavior, and even when you do, you still get the feeling that something is amiss. Yet, I certainly wouldn't pass up the opportunity to do dissections, and I know my classmates feel the same way.
Even though we've only had one dissection (two more this week; not sure what we did to earn this punishment), I've already learned a great deal. We started with the back because the muscles are large and it's relatively difficult to screw it up. To get to the good stuff however, required several hours of removing fat from the body spaces. Our body, unfortunately, is quite obese, which essentially acts to increase the amount of time it takes us to remove unimportant parts and ramps up the difficulty in defining the stuff we do want to keep. The other problem with dissection is that most anatomy atlases are color coded. This is great for learning initially, but completely useless for the cadaver. Normal living tissue retains some of its color, but the cadavers are mostly shades of gray. And since part of our grade comes from identifying structures on cadavers, it's kind of a big deal to know what areas you are dealing with.
I'm going to try to touch on some non-med school related topics this week, but we'll see how that actually goes. Now that we're done with orientation, our schedule is a little more regular. Apparently things don't really die down until the spring semester though, so I'm SOL at the moment. Is it too late to change to business school?
I'm going to try to touch on some non-med school related topics this week, but we'll see how that actually goes. Now that we're done with orientation, our schedule is a little more regular. Apparently things don't really die down until the spring semester though, so I'm SOL at the moment. Is it too late to change to business school?
Saturday, August 18, 2012
Applying to Medical School: Skillful Interviewing
For those of you applying to medical school, we're nearing the point where the first interviews will begin. Typically, the first invites go out in late July/August, and the first interviews are in September. Each school is different, particularly depending on when the secondary application goes out. Anyways, the interview is probably the most important part of the admissions process. Why? If a school gives you an interview, they're already pretty interested in you. Remember, only 10-20% of applicants to a school are interviewed. You already beat out a large portion of people. Now you have to land the deal.
In terms of helping or hurting you, the interview can do both, but to different levels. My opinion is that, a good interview will help you a little, but a bad interview will hurt you a lot. Think of it this way: You are like a cake. When you go to interview, the admissions committee is looking to confirm that you are what they want. They are checking to see if the cake is ready and looks good. Your individual talents/personality is the frosting or sprinkles or design that sets the cake apart from others. However, if they find your cake lacking in substance or taste, no matter how much frosting you put on it, no one will want to eat it.
So, how do you make sure you present your best, most tastiest cake? First and foremost, acknowledge that there is a great degree of luck involved. For example, on one interview, my interviewer and I had a lot in common. As a result, the interview flowed nicely from topic to topic, and we both had fun (at least I did). That was the luck factor; so much is dependent on who your interviewer is and how he/she is feeling that day, among other things. Don't despair though! You can still nail the interview by doing a few simple things.
1. Look nice. Make sure you are dressed nicely (suit is highly recommended) and well groomed. Medicine is fairly conservative (at least the interview part), so don't go overboard on make-up or fashion.
2. Be comfortable and relaxed. Okay, realistically you'll be pretty anxious; I was too. Just try not to let it show too much. Do some deep breathing exercises if you find yourself getting too worked up. And don't be afraid to take a second or two to think about a question before you respond. You want your sentences to be of substance; talking more doesn't necessarily mean better. Also, I recommend you wear your suit a couple times before your interview day. You can tell who is wearing a suit for the first time because they tend to look uncomfortable. So dress up to class or work a couple times to get used to the feel.
3. Be polite and positive. This goes without saying. Be polite to everyone, especially the staff and other interviewees. You never know when you are being observed...
4. Be passionate, be genuine, and know your application material. This is crucial. You will probably be asked about your application (some interviews are different, like the MMI). Make sure you can spend at least a few minutes talking about anything you mentioned. Most importantly, make sure you speak enthusiastically. Now, you don't want to go used-car-salesman on your interviewer, but make sure you convey a degree of excitement about the things you mentioned in your application. Look, everyone knows there is a great deal of scut work you have to do to get into med school. Just don't present that way. If you did research, talk about it. If you had a powerful experience volunteering or on a trip, explain how it impacted you so heavily. It's not the smartest, most accomplished people who get into medical school. It's the ones who show that they want it most, that they're willing to put in the effort to succeed. Make damn sure you get that point across.
5. Send a thank you note. For the love of all things good, write down the name of your interviewer(s) so you can send a thank you note. Often times you'll send it to the admissions office, and they can forward it to the person. Very important you do this. It doesn't have to be long (mine was a couple sentences saying thank you and mentioning a specific thing we talked about to make it seem less generic), but it's important you do this follow up.
You can find interview tips just by doing a simple Google search, so I encourage you to look up those general pointers. Honestly, the medical school interview is a lot of fun. It's the closest you'll be to getting into med school. You'll get to talk to students, find out about the curriculum, maybe even sit in on a lecture (if you get the option to stay with a student host, do it. It's way better than staying in a hotel. Just trust me on this one). The interview is the final hurdle you have to get over. There is essentially nothing left to do afterwards except wait for a decision. You can send update letters or interest letters to the school, but make sure you actually have something substantial to say. Avoid calling the office to see if a decision is made; you'll find out in due time. Most importantly, relax a bit. You got through it all! If all goes well, you'll get that beautiful, wonderful acceptance letter (and often phone call) in no time.
So remember, have fun. It's a long, tedious, stressful process, but if you stay positive and make the most of it, it'll reflect in your application, and good things will happen.
So, how do you make sure you present your best, most tastiest cake? First and foremost, acknowledge that there is a great degree of luck involved. For example, on one interview, my interviewer and I had a lot in common. As a result, the interview flowed nicely from topic to topic, and we both had fun (at least I did). That was the luck factor; so much is dependent on who your interviewer is and how he/she is feeling that day, among other things. Don't despair though! You can still nail the interview by doing a few simple things.
1. Look nice. Make sure you are dressed nicely (suit is highly recommended) and well groomed. Medicine is fairly conservative (at least the interview part), so don't go overboard on make-up or fashion.
2. Be comfortable and relaxed. Okay, realistically you'll be pretty anxious; I was too. Just try not to let it show too much. Do some deep breathing exercises if you find yourself getting too worked up. And don't be afraid to take a second or two to think about a question before you respond. You want your sentences to be of substance; talking more doesn't necessarily mean better. Also, I recommend you wear your suit a couple times before your interview day. You can tell who is wearing a suit for the first time because they tend to look uncomfortable. So dress up to class or work a couple times to get used to the feel.
3. Be polite and positive. This goes without saying. Be polite to everyone, especially the staff and other interviewees. You never know when you are being observed...
4. Be passionate, be genuine, and know your application material. This is crucial. You will probably be asked about your application (some interviews are different, like the MMI). Make sure you can spend at least a few minutes talking about anything you mentioned. Most importantly, make sure you speak enthusiastically. Now, you don't want to go used-car-salesman on your interviewer, but make sure you convey a degree of excitement about the things you mentioned in your application. Look, everyone knows there is a great deal of scut work you have to do to get into med school. Just don't present that way. If you did research, talk about it. If you had a powerful experience volunteering or on a trip, explain how it impacted you so heavily. It's not the smartest, most accomplished people who get into medical school. It's the ones who show that they want it most, that they're willing to put in the effort to succeed. Make damn sure you get that point across.
5. Send a thank you note. For the love of all things good, write down the name of your interviewer(s) so you can send a thank you note. Often times you'll send it to the admissions office, and they can forward it to the person. Very important you do this. It doesn't have to be long (mine was a couple sentences saying thank you and mentioning a specific thing we talked about to make it seem less generic), but it's important you do this follow up.
You can find interview tips just by doing a simple Google search, so I encourage you to look up those general pointers. Honestly, the medical school interview is a lot of fun. It's the closest you'll be to getting into med school. You'll get to talk to students, find out about the curriculum, maybe even sit in on a lecture (if you get the option to stay with a student host, do it. It's way better than staying in a hotel. Just trust me on this one). The interview is the final hurdle you have to get over. There is essentially nothing left to do afterwards except wait for a decision. You can send update letters or interest letters to the school, but make sure you actually have something substantial to say. Avoid calling the office to see if a decision is made; you'll find out in due time. Most importantly, relax a bit. You got through it all! If all goes well, you'll get that beautiful, wonderful acceptance letter (and often phone call) in no time.
So remember, have fun. It's a long, tedious, stressful process, but if you stay positive and make the most of it, it'll reflect in your application, and good things will happen.
Sunday, August 12, 2012
Return From Hiatus, With A Bright White Coat
Despite having nearly nothing to do for the past few weeks, I just could not find time to write a new post. It is truly a tragedy. Anyways, some things have changed since we last spoke. Most notably, I have made the transition from premed student to medical student. This was accomplished through a symbolic and somewhat odd ceremony called the White Coat Ceremony. Like a mini-graduation, several of the deans spoke to us and our family/friends/passing hobos about the significance of the occasion and offered advice about how to proceed forward. Then, four at a time, we are called up to the stage and "coated" by one of the deans. This was followed by a recitation of a modified version of the Hippocratic Oath, which was followed (I think) by drinking.
The odd part of the ceremony was two-fold. First, it was inordinately humid out, so everyone was drenched in sweat by the time we finished. Secondly, it seemed strange to hold such an elaborate celebration before we actually accomplished anything. Don't get me wrong, we all got into med school, which is a feat on its own. But I think the ceremony would make more sense between the 2nd and 3rd year. That's the bigger transition, when you go from student in lecture to student in practice.
Regardless, the start of school is still something to be excited about. Unfortunately, most of the week was spent in orientation type events, so we've yet to dive in deep (that changes starting tomorrow). So, what do I have on my plate for the next few months? Well, I've got your standard biochemistry and anatomy courses. We also have two courses in public health and human behavior, one each. Finally, we have a couple clinical med and problem based learning courses. At first glance, it may seem like your ordinary (difficult) college schedule. The deceptive part is that we have multiple lectures per subject per day. For example, tomorrow I have a three hour anatomy block, followed by two hours of lectures in biochem and another 1.5 hour public health lecture. That's how they get you. I have 6 hours of biochem, 9 hours of anatomy (lab starts next week), 8.5 hours of public health, and 3 hours of behavior. And that's just lecture time; many more hours of study are required for mastery. I'm starting to get that fire hose analogy now.
Anyways, I'll try to do better about posting. Maybe I'll even get on a schedule. Consistency is key! Here's to the start of an exciting four years!
Saturday, July 21, 2012
We All Spend Time As A Shadow
I leave my apartment and hop in the car, already feeling a little drowsy. It's 10:30 pm, and I'm heading to work. In order to satisfy a requirement for an internship, I scheduled two ED shadowing shifts back to back, starting at 11pm and going till 7am. I took two shifts previously from 6pm to 2am, but this was different. Going to work in the middle of the night feels unnatural, though the commute is pretty good. I arrive at the hospital, carrying my coffee-filled thermos (essential), ready for the night shift.
So, you want to be a doctor. Fantastic (although if I had a nickel for every time I heard that, I wouldn't be taking out so many loans for med school). What does a doctor do? If you answered "Helps people" you are probably a freshman with good intentions but much naïveté. If you chose "Paperwork" or "Sitting at a computer" you probably have a little more experience. If you said "Inflict pain and interrupt frequently" you are probably a patient. Most people have a general idea of what physicians do, but they lack the important day-to-day details. Medicine is fairly romanticized thanks in large part to shows like ER, House, or Grey's Anatomy, and the many that came before it. Watching people put in orders, review charts, wait for labs, or conduct rounds does not make for very interesting TV (to the general public at least). Thus we arrive at our stereotypical freshman pre-med, gunning for med school without any conception of what physicians actually do. This is where shadowing comes in.
The ED is arranged like a giant horseshoe, the interior being the nurses' and physician's stations and the exterior being the patient rooms. I set my coffee down and put my snack in the mini-fridge (god help you if you fail to bring snacks). I greet Dr. S. and we begin the night. Dr. S. is very mild mannered and speaks calmly (ER docs tend to come from both ends of the spectrum, calm and manic). It is a typical night at the ER; abdominal pain is coming at us from every direction and shows no sign of letting up. Not too far into the shift, an elderly woman arrives by EMS. She was unconscious and had some dried blood on her head, suspicious for a fall. She was weakly responsive to pain, but no spontaneous movement or sounds. She got the usual 'ER Special' consisting of IVs, blood tests, and cardiac monitoring. She would almost certainly be admitted. Neurology would be consulted as soon as possible. Several hours later, her daughter came running out of the room, shouting for help; the patient was having a seizure. After a tense minute or two of not being able to locate any nurses or Dr. S. (he is the only physician on at this point), we stream into the room to assess the situation. The patient has stopped seizing at the moment, but is now not breathing. Her heart rate plummets. Quickly, a nurse starts to bag her, and Dr. S. makes the decision to intubate. Respiratory is paged, and a nurse prepares anti-convulsants. Finally, she's stabilized, and we all go back to work. No rest for the weary.
Shadowing is exactly as it sounds: the student follows the physician like a shadow, in order to observe. However, unlike a shadow, you will constantly be in the way, and you can/might be allowed to ask questions. Medical students are expected to ask questions, even if they end up being forced to answer their very own questions and ultimately being chastised for not knowing the answer (doesn't seem fair does it). It is extremely useful though, because you gain firsthand knowledge of how a typical day/shift goes. For example, I was shadowing an ER doc, and for the first 2-3 hours, we didn't see one patient. Labs were backed up and beds were full, so we just sat on our asses until it cleared out a bit. You do get to see procedures and patients (especially in surgery), but the little things are actually the most important. Adcoms want to see that you know what you're in for; the fairy-tale can be your motivation, but you better be prepared for the reality.
Around 5am or so, Dr. S. are seeing a patient about back pain when the intercom clicks on. "All help to triage stat!" the nurse shouts (first time I heard stat used in a serious context). Dr. S. is not phased, and continues to interview the patient. Seconds later, "Physician to triage!" Dr. S. sighs, apologizing to the patient, and we head down the hall to the waiting room (slowly I might add). Before we get there, two beds complete with patients come flying around the corner, pushed by a couple personnel. Both patients were stabbed at a party and had just walked in the front door. Minutes later, a third patient comes in and is wheeled back to an empty bed. The ED goes into lock-down, police are called, vitals and IVs are started, and ambulances are called to transfer the patients (the hospital is not a trauma facility). Shortly after our three stab victims arrive, a code blue goes out over the intercom. The physician covering the wards, Dr. P., is currently in the ED, and Dr. S. is not sure if she's even ACLS certified. Dr. S. and his scribe take off after her with the code box, and I am tasked with getting vitals from the patients. They all appear to be in discomfort, but one looks very pale and is shaking (effects of epinephrine). Dr. S. and his now disheveled looking scribe (CPR will do that to you) return, and the patients are transferred.
So, shadowing is important, an unwritten requirement of medical school. But how do you go about it? I was lucky; I got an internship through the university that handled the initial contact. For those less fortunate, I would suggest asking around the hospital if you volunteer at one. Academic medical centers are probably the best choice because they will be used to having medical students around. Ask your friends too. I came from a completely non-medical family, so I was at a bit of a disadvantage. Many of my friends had physician parents or grandparents, so they became a great source of knowledge. There are lots of guides pertaining to shadowing though, so just search SDN or Google for more in depth advice. You don't have to rack up hours and hours of shadowing, but spend one or two full shifts per specialty. It helps to get some variety as well, but even one experience is better than none. Don't forget to have fun, but make sure you reflect on your experiences too. If you really can't see yourself living that life, it might be time to switch paths. That's what shadowing is for. It wipes away some of the glamour, exposing the realism of clinical practice. It disenchants, leaving only the most dedicated behind to finish the journey to medical school.
The ED is arranged like a giant horseshoe, the interior being the nurses' and physician's stations and the exterior being the patient rooms. I set my coffee down and put my snack in the mini-fridge (god help you if you fail to bring snacks). I greet Dr. S. and we begin the night. Dr. S. is very mild mannered and speaks calmly (ER docs tend to come from both ends of the spectrum, calm and manic). It is a typical night at the ER; abdominal pain is coming at us from every direction and shows no sign of letting up. Not too far into the shift, an elderly woman arrives by EMS. She was unconscious and had some dried blood on her head, suspicious for a fall. She was weakly responsive to pain, but no spontaneous movement or sounds. She got the usual 'ER Special' consisting of IVs, blood tests, and cardiac monitoring. She would almost certainly be admitted. Neurology would be consulted as soon as possible. Several hours later, her daughter came running out of the room, shouting for help; the patient was having a seizure. After a tense minute or two of not being able to locate any nurses or Dr. S. (he is the only physician on at this point), we stream into the room to assess the situation. The patient has stopped seizing at the moment, but is now not breathing. Her heart rate plummets. Quickly, a nurse starts to bag her, and Dr. S. makes the decision to intubate. Respiratory is paged, and a nurse prepares anti-convulsants. Finally, she's stabilized, and we all go back to work. No rest for the weary.
Shadowing is exactly as it sounds: the student follows the physician like a shadow, in order to observe. However, unlike a shadow, you will constantly be in the way, and you can/might be allowed to ask questions. Medical students are expected to ask questions, even if they end up being forced to answer their very own questions and ultimately being chastised for not knowing the answer (doesn't seem fair does it). It is extremely useful though, because you gain firsthand knowledge of how a typical day/shift goes. For example, I was shadowing an ER doc, and for the first 2-3 hours, we didn't see one patient. Labs were backed up and beds were full, so we just sat on our asses until it cleared out a bit. You do get to see procedures and patients (especially in surgery), but the little things are actually the most important. Adcoms want to see that you know what you're in for; the fairy-tale can be your motivation, but you better be prepared for the reality.
Around 5am or so, Dr. S. are seeing a patient about back pain when the intercom clicks on. "All help to triage stat!" the nurse shouts (first time I heard stat used in a serious context). Dr. S. is not phased, and continues to interview the patient. Seconds later, "Physician to triage!" Dr. S. sighs, apologizing to the patient, and we head down the hall to the waiting room (slowly I might add). Before we get there, two beds complete with patients come flying around the corner, pushed by a couple personnel. Both patients were stabbed at a party and had just walked in the front door. Minutes later, a third patient comes in and is wheeled back to an empty bed. The ED goes into lock-down, police are called, vitals and IVs are started, and ambulances are called to transfer the patients (the hospital is not a trauma facility). Shortly after our three stab victims arrive, a code blue goes out over the intercom. The physician covering the wards, Dr. P., is currently in the ED, and Dr. S. is not sure if she's even ACLS certified. Dr. S. and his scribe take off after her with the code box, and I am tasked with getting vitals from the patients. They all appear to be in discomfort, but one looks very pale and is shaking (effects of epinephrine). Dr. S. and his now disheveled looking scribe (CPR will do that to you) return, and the patients are transferred.
So, shadowing is important, an unwritten requirement of medical school. But how do you go about it? I was lucky; I got an internship through the university that handled the initial contact. For those less fortunate, I would suggest asking around the hospital if you volunteer at one. Academic medical centers are probably the best choice because they will be used to having medical students around. Ask your friends too. I came from a completely non-medical family, so I was at a bit of a disadvantage. Many of my friends had physician parents or grandparents, so they became a great source of knowledge. There are lots of guides pertaining to shadowing though, so just search SDN or Google for more in depth advice. You don't have to rack up hours and hours of shadowing, but spend one or two full shifts per specialty. It helps to get some variety as well, but even one experience is better than none. Don't forget to have fun, but make sure you reflect on your experiences too. If you really can't see yourself living that life, it might be time to switch paths. That's what shadowing is for. It wipes away some of the glamour, exposing the realism of clinical practice. It disenchants, leaving only the most dedicated behind to finish the journey to medical school.
Sunday, July 15, 2012
Know The Difference: Heart Attack vs Cardiac Arrest
Welcome to the second installment of "Know the Difference," a series which seeks to clear up common medical misnomers. This week, we're tackling a one of the most prominent naming errors on television (and by extension, the public). The scene is a hospital room, with the patient lying in the bed looking quite unhappy and ill. In walk our doctors, who bear an uncanny resemblance to team featured on House. They chat with the patient briefly, exchange some comical banter with each other, and then the patient takes a turn for the worse. The camera pans up to the cardiac monitor, which shows a complete asystole (flat line). Everyone springs dramatically into action, but one of the doctors commits a medical student faux paus. "She's having a heart attack!" he exclaims, sending a brief jolt of pain to the frontal lobes of the clinical staff watching at home.
So what happened? Basically the hotshot doctor was confusing two conditions, heart attack and cardiac arrest. And since they are treated very differently, it is kind of a big deal to get it right. So how do you tell one from the other?
A cardiac arrest (CA) occurs when the heart is no longer pumping blood. This is determined clinically by checking for a pulse. If it is absent, congratulations; you now have a genuine emergency on your hands. When the heart stops pumping blood, oxygen and nutrients cannot circulate through the body, and waste begins to build up. Without intervention, CA is fatal in a matter of minutes (predominantly due to the lack of oxygen)(1). CA is treated differently depending on the cause and EKG interpretation. For instance, the most common one seen on TV is asystole:
So what happened? Basically the hotshot doctor was confusing two conditions, heart attack and cardiac arrest. And since they are treated very differently, it is kind of a big deal to get it right. So how do you tell one from the other?
A cardiac arrest (CA) occurs when the heart is no longer pumping blood. This is determined clinically by checking for a pulse. If it is absent, congratulations; you now have a genuine emergency on your hands. When the heart stops pumping blood, oxygen and nutrients cannot circulate through the body, and waste begins to build up. Without intervention, CA is fatal in a matter of minutes (predominantly due to the lack of oxygen)(1). CA is treated differently depending on the cause and EKG interpretation. For instance, the most common one seen on TV is asystole:
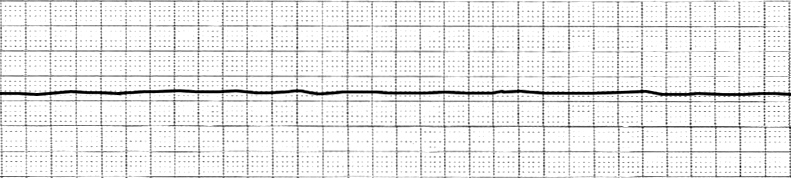 |
| Asystole. Note no discernible waves. Courtesy of wikipedia. |
This is also the most common rhythm seen in Out-of-Hospital arrests(2). Asystole has a number of causes, some reversible some not. Typically, this rhythm is seen after prolonged pulselessness, so the prognosis is grim. The treatment usually involves reversing the underlying condition (toxicity, tamponade, tension pneumo, etc). What it does not involve is electrical shocks. Asystole is not a shockable rhythm. So, while making for very good television, our team of doctors would not be doing any good with the defibrillator in the typical case. Ventricular fibrillation (V-fib or VF) on the other hand, is shockable, even though it may not look like an abnormal rhythm to the untrained eye.
 |
| V-fib. Only random waveforms. Also courtesy of wikipedia. |
VF is a pulseless rhythm where the heart is contracting randomly, out of sync.
A heart attack (MI) is also a serious condition, but does not lead to death per se. An MI occurs when blood flow to the heart is reduced, classically causing chest pain (angina) and dyspnea(2). The reduction of blood flow is usually due to a narrowing in one or more of the coronary arteries. Thus, the primary intervention is to open the arteries back up (PCI) or bypass blocked portions (CABG). The main difference between MI and CA is that cardiac arrest is a complication of an MI. If the blood flow is cut off for too long, heart muscle (myocardium) will die. This can lead to arrhythmias or heart failure, which may lead to death. The EKG of a person having a heart attack can vary substantially, but here are some examples of anterior MIs.
Summary
CA: No pulse, heart is not pumping blood. Rapidly fatal. Treatment (resuscitation) depends on the rhythm appearance.
MI: Reduced blood flow to the heart via the coronary arteries. Muscle death may impair normal function of the heart and lead to death.
So the next time you're watching House or Gray's Anatomy (or ER for the slightly older readers), keep an eye on that monitor and get ready to call those actors out on their mistakes!
Sources
1.CPR - adult. PubMed Health. 2011. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001083/. Accessed July 15, 2012.
2. Mader TJ, et al. Out-of-hospital cardiac arrest outcomes stratified by rhythm analysis. Resuscitation (2012), http://dx.doi.org/10.1016/j.resuscitation.2012.03.033.
3. Heart Attack. PubMed Health. 2011. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001246/. Accessed July 15, 2012.
Monday, July 2, 2012
Behavior's Big Bang Theory
First, I'd like to say my alliteration skills are still spot on. Second, this has nothing to do with the popular TV show, The Big Bang Theory. Sorry to disappoint (secretly I hope I tricked you, and you'll decide to stay anyways).
When I spoke about behavior last time, my discussion was mostly limited to defining what it is and how we look at it. To recap, a behavior is anything you do to solve an adaptive problem, and we categorize it functionally rather than structurally. For example, opening a jar of pickles solves the adaptive problem of getting food, but we don't care exactly how you opened it. You could have twisted the lid off like the majority of individuals (let's be honest, the majority of individuals actually gave it to someone else to open), but you also could have hit the jar with a sledgehammer or treated it to some explosives a la Mythbusters. Each of these techniques would have opened the jar, but some work better than others. The twisting method is quick, easy to do, and requires minimal energy. Blowing up the jar is more pleasing to the senses, but it requires access to explosives and time to set them up, generates new adaptive problems (flying shrapnel, angry neighbors, destroyed kitchen, etc), and probably obliterates the pickles in the process. So, the next two logical questions to ask are, "Where does behavior come from?" and "How do we find the right one for the job?"
Now, when we ask for the origins of behavior, we are really asking, "What causes behavior?" There are several answers to this depending on your frame of reference. Physiologically, behavior arises as an emergent property (epiphenomenon if you will) from the behavior of multiple neurons (and their effector organs) working together. I would be more specific if I could, be we actually have not yet identified most behaviors to particular networks of neurons. If you filled a backpack with headphones, the resulting tangled mess would give you a good analogy for the complexity of the brain. Untangling the mess is the job of neuroscientists, neuropsychologists, and basically anyone whose title starts with neuro. Behaviorists such as myself stick to the macroscopic world (but we still find the microscopic interesting), dividing our causes into two categories: proximate and ultimate. A proximate cause is the immediate antecedent to the behavior. For the behavior of answering the phone, the proximate cause is the phone ringing. The ultimate cause is more difficult to explain, but suffice it to say, determines why you behave due to a history of reinforcement. For example, you have to drive from Point A to Point B. You take route #1, but it's rush hour and it takes a long time to get there. After doing this several times, you take route #2. It is still rush hour, but you get from A to B much faster. Now the weekend comes. You take route #1 and get to point B in about the same amount of time as route #2, even though it's the same time of day. Gradually, your response is shaped to taking route #2 during rush hour and route #1 during weekends. The route you take (response) due to rush hour + time of day (cues) is a result of a history of reinforcement. If someone asked you why you took route #2 during rush hour, your response summarizes the ultimate cause (It is faster than route #1). So, the proximate cause explains why you behaved in one way as opposed to another, and the ultimate cause explains how you developed that way of behaving.
The mistake most people make when talking about behavior is dismissing the ultimate cause. When a guy in line at the coffee store yells at the person serving his coffee, you may be tempted to say, "He yelled at the worker because he is a jerk." That explains everything right? Jerks yell at people; it makes sense. Unfortunately, by doing that, you fell into B.F. Skinner's 3rd circle of Hell. Your reasoning is actually circular reasoning; he yelled at the worker because he is a jerk, and the guy is a jerk because he yelled at the worker. The ultimate cause is much less visible, having occurred in the past and over a period time, so it is very easy to miss. Additionally, the ultimate cause may be a product of evolution, further obscuring it. Widespread obesity can be attributed to physiologic mechanisms that evolved to prevent starvation (epitomized in meme form as, "Eat all the things!").
At this point, I've provided a partial explanation for the origin of behavior. Tune in next time for the epic finale.
Subscribe to:
Comments (Atom)